References:
- Kozier & Erb’s Fundamentals of Nursing: Concepts, Process, and Practice, 11th Edition, ISBN 9780135428733, by Audrey Berman, Shirlee J. Snyder, and Geralyn Frandsen (Ch. 28, pp. 532–569)
Body temperature is the balance between heat generation and heat loss. In general, there are two types of body heat: core temperature, measured through contact with mucous membranes or directly from organs or muscles, and surface temperature, measured through the skin.
Heat Production
The body’s metabolism is the primary dictator of heat production. The basal metabolic rate itself is the baseline level of metabolism in individuals. Cellular metabolism increases with more muscle activity (exercise, shivering, etc.), higher hormonal function (T₄, epinephrine, and norepinephrine), and other biological functions such as inflammation and fever.
- Age also plays a role in heat production; heat production is generally high in younger ages and gradually decreases as one approaches late adulthood.
Heat Loss
- Radiation: the transfer of heat without direct contact, such as the warmth felt from the sun despite its distance from us.
- Conduction: the transfer of heat through contact.
- Convection: the transfer of heat through contact through drafts and wind— air currents.
- Evaporation: the loss of heat as moisture evaporates from the surface of the body, which carries heat away from the body. This occurs in breathing, exposed mucosa like the mouth, and importantly, sweating.
Multiple factors affect body temperature outside of the body’s biological processes. Variance in body temperature may even be explained through these normal conditions:
- Age: infants and children have greater variances in temperature compared to pubertal children and adolescents/adults. As mentioned earlier, metabolic processes continue to slow into adulthood, with those over 75 years old being at risk for hypothermia and hyperthermia. This occurs as a result of both thermoregulatory and physiologic changes.
- Diurnal Variations: temperature undergoes elevations and depressions in line with an individual’s circadian rhythm. “Diurnal” refers to day time, opposite of “Nocturnal”. The body temperature is normally the lowest from 0400 to 0600 hours and rise by up to 1.0°C at the peak, usually around 1600 and 1800 hours (a 12 hour-cycle).
- Stress: stimulation of the sympathetic nervous system can increase metabolic activity and heat production. Stressed and anxious patients are anticipated to have elevated body temperatures.
- Environment: extremes in environmental temperature can affect a client’s thermoregulatory systems.
Thermoregulation
The hypothalamus (“hypothalamic integrator”) maintains the body’s optimal temperature by working with sensory receptors throughout the body (peripheral and core). These sensors detect cold and warmth and apply physiologic processes accordingly:
- When cold is detected, (a) shivering, rapid contraction and relaxation of skeletal muscles, occurs to produce heat from muscle activity, (b) sweat inhibition to decrease evaporative heat loss, and (c) vasoconstriction to decrease heat loss by distancing the blood from the skin, allowing it to stay “inside”.
- When warmth is detected, the opposite occurs; (a) sweating increases to enhance evaporative cooling, and (b) peripheral vasodilation occurs.
The conscious mind also experiences discomfort with these temperatures and takes steps to thermoregulate, such as through clothing in response to cold or using a fan in response to heat.
Alterations in Body Temperature
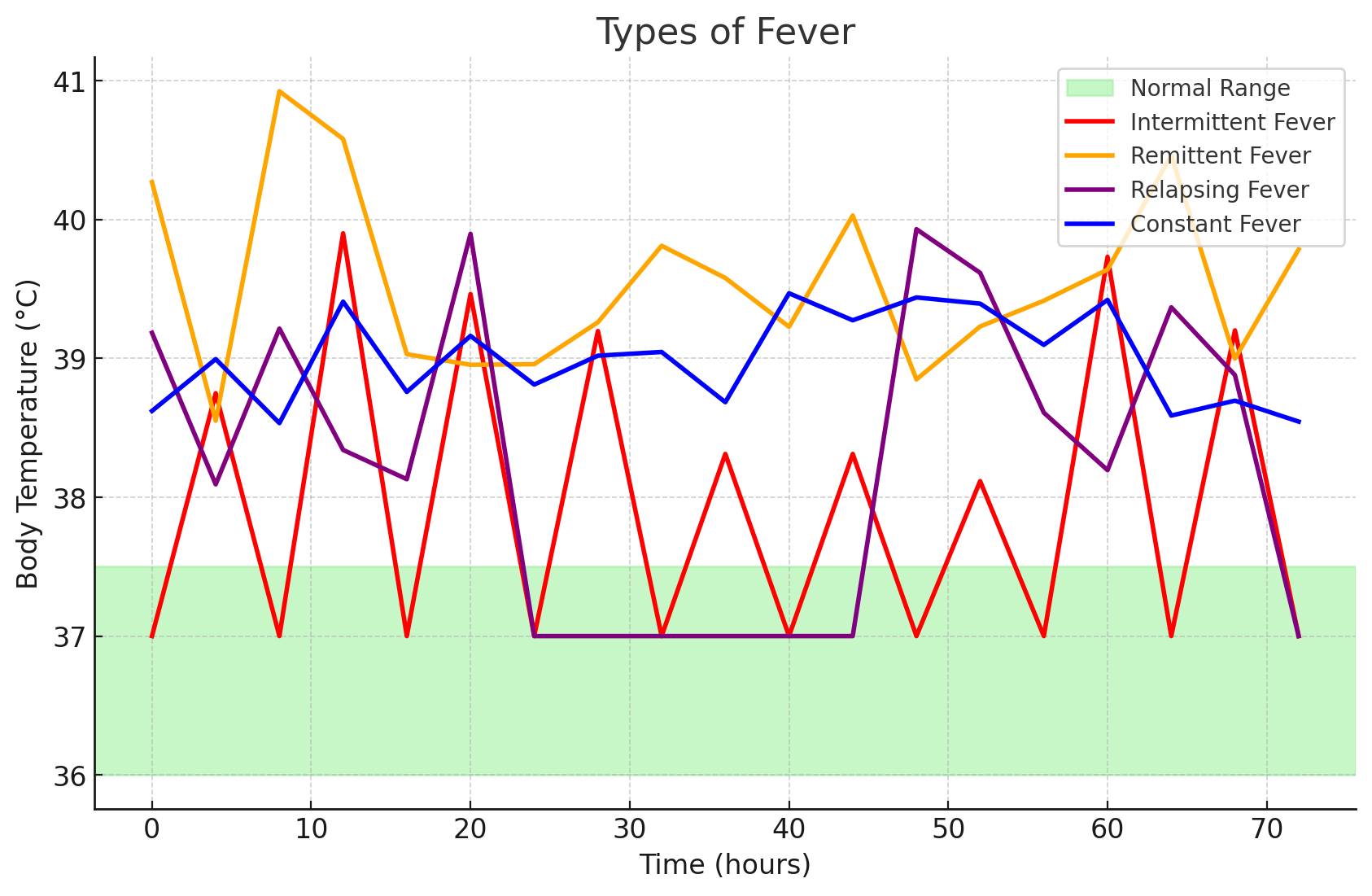
Some declarations: normal temperature is considered to be between 36°C and 37.5°C (96.8°F to 99.5°F). Any temperature higher than this is considered pyrexia (“hyperpyrexia” if ≥41°C) and any temperature is considered hypothermia.
-
Intermittent Fever: an intermittent fever is one whose temperature alternates between normal temperature and hyperthermia within one day. Common examples of this includes malaria and pulmonary tuberculosis.
-
Remittent Fever: a fever that maintains a high temperature with wide fluctuations (>2°C) over 24 hours.
-
Relapsing Fever: a fever with short periods (one to two days) of normal body temperature.
-
Constant Fever: a fever that maintains a high temperature with small fluctuations in temperature (<2°C) over 24 hours.
-
Fever Spikes: temperatures that rapidly become feverish then returns to normal within a few hours, often due to bacterial blood infections.
-
Heat Exhaustion: a source of high temperature that is not a “true” fever caused by biological processes; it is a result of environmental exposure. This is accompanied by paleness, dizziness, nausea, vomiting, fainting, and a moderately increased temperature (38.3°C to 38.9°C [101°F to 102°F]). Higher yet (~41.1°C), the individual stops sweating and the skin feels warm and appears flushed. The individual becomes delirious, potentially becomes unconscious, and may experience seizures. This is a heat stroke.
-
Hypothermia: a result of excessive heat loss, inadequate heat production, and impaired hypothalamic thermoregulation. This may be accidental or induced to decrease the oxygen requirement by body tissues such as during certain surgeries. In accidents (exposure to cold environment, immersion in cold water, lack of adequate clothing or heat source), skin and underlying tissues may be damaged by the freezing cold, resulting in frostbite. This commonly occurs in hands, feet, nose, and ears. Patients with hypothermia display decreased body temperature, pulse, respirations, blood pressure, urine output, and level of consciousness progressing down to a coma; severe shivering in early stages; feeling of cold and chills; pale, cool, waxy skin; and lack of muscle coordination.
- Managing hypothermia involves removing the client from the cold and rewarming the client’s body. (a) Mild Hypothermia can be managed with blankets, (b) Severe Hypothermia should be managed with hypothermia blankets and warm IV fluids. A warm environment, dry clothing and head cover, positioning (limbs close to body), warm oral fluids, and warming pads are all methods for rewarming the patient.
Frostbite
- First Degree Frostbite: the skin is intact; it is often only reddened— circulation is intact.
- Second Degree Frostbite: frost has penetrated into the epidermis.
- Third Degree Frostbite: frost has penetrated into the subcutaneous tissue.
- Fourth Degree Frostbite: tissue has become necrotic and blackened.
Assessing Body Temperature
| Site of Measurement | Heat Type and Reference Range | Considerations | Placement |
|---|---|---|---|
| Oral Temperature | Core; 36.5 - 37.5°C | Accessible and convenient. - Patient must be awake and oriented. - This is only used for patients 3 years old and above. - The bulb of the thermometer is placed sublingually, in contact with the side of the frenulum. - Thermometers can break if bitten - Inaccurate if client has just ingested hot or cold food or fluid or smoked. The nurse must wait 30 minutes before taking an oral temperature. - Could injure the mouth following oral surgery. | The tip of the thermometer is placed on either side of the frenulum. |
| Rectal Temperature | Core; +1°C of oral | Reliable; very accurate. - Clean gloves are used. - Insertion is done during inhalation when the sphincter relaxes. Insertion is 1.5” to 2” for adults and 0.5” to 1” for children. - Inconvenient and more unpleasant for clients; difficult for clients who cannot turn to the side. - Could injure the rectum. Contraindicated for rectal surgery, diarrhea, immunosuppression, and clotting disorders/hemorrhoids. - Presence of stool may interfere with thermometer placement. | Apply clean gloves and instruct the client to take a slow deep breath during insertion. Never force the thermometer if resistance is felt. |
| Axillary Temperature | Surface; -1°C of oral; least accurate reading | Safe and noninvasive. Preferred for newborns. This is usually only recommended for adults for whom other temperature sites are contraindicated. - The axilla must be dry (pat dry if damp). Hair may also be a problem. - The thermometer may need to be left in place a long time to obtain an accurate measurement. | Pat the axilla dry if very moist. The tip of the thermometer is placed in the center of the axilla. |
| Tympanic Temperature | Core; +0.3°C | Readily accessible; reflects the core temperature; very fast - A fast and accurate method of taking temperature, often used in children. However, it may be uncomfortable, injurious, and affected by cerumen. - Straightening of the ear canal is required for a reading. For children up to three years of age, pull the ear back and down. If older, pull the ear back and up - Can be uncomfortable and involves risk of injuring the membrane if the probe is inserted too far. - Repeated measurements may vary. Right and left measurements can differ if there are anatomic or pathologic differences (e.g., infection). - Presence of cerumen can affect the reading. - Requires proper technique; not too loose nor tight in the use of the probe. | Pull the pinna slightly upward and backward (adult) while inserting the tympanic thermometer. The probe is pointed slightly anteriorly towards the eardrum, and inserted slowly using a rotating motion until snug. |
| Temporal Temperature | Surface; Same as core temperature. | Safe and noninvasive; very fast. May utilize a patch, chemical thermometer, or temporal artery thermometer. This is useful for infants and children. - Requires electronic equipment that may be expensive or unavailable. Variation in technique needed (forehead-temple) if the client has perspiration on the forehead. | Brush hair aside if covering the temporal artery area. The probe is placed flush midline on the forehead and slowly slid to the hairline, not down the side of the face, then touch it on the neck just behind the earlobe. |
Mercury Thermometer Breakage
In the event of the breakage of a mercury thermometer, the nurse requires proper disposal protocol to avoid mercury poisoning. The nurse requires (a) any rubber gloves, (b) paper towels to soak up the mercury, (c) plastic bags for disposal sealed with tape, and (d) a flashlight to scan for beads of mercury. All contaminated materials must be disposed. Disposal via drain and vacuuming and sweeping are dangerous.
Any mercurial thermometers encountered should be promptly recommended for replacement and safe disposal.
Temperature Scales
Kozier utilizes three mathematical operations to translate between Celsius and Fahrenheit: (a) a constant subtraction or addition of 32, and (b) multiplication by or .
Personally, I replace or with , and instead change between division and multiplication—°C is smaller than °F, so converting from °F to °C uses subtraction then division; °F is larger than °C, so converting from °C to °F uses multiplication then addition. Whichever is easier to remember for you. 🤷♂️
Temperature Assessment Procedure
Assessing body temperature is done to:
- Establish baseline data.
- Evaluating deviations of core temperature.
- Evaluating changes in core temperature in response to specific therapies.
- Monitoring clients at risk for imbalanced body temperature.
| Phase | Nursing Activities |
|---|---|
| Assessment | Check for clinical signs of fever and hypothermia, appropriate sites for assessment, and factors that may alter core body temperature. |
| Planning | Assign: routine measurements may be delegated to APs or even family members or caregivers in nonhospital settings. The nurse bears the responsibility of educating delegates for the type of thermometer to use, site to use, how to record findings, and when to report abnormal temperatures to the nurse. The nurse interprets abnormal temperatures and determines appropriate responses. Equipment: thermometer and its sheath or cover, water-soluble lubricant (if rectal), towel (if axillary), and tissues or wipes. |
| Implementation | Make sure all gathered equipment are functioning normally. Prior to performing the procedure, the nurse must introduce themselves and verify the client’s identity using agency protocol. Explanation of the nurse’s purpose, the procedure, and how the patient will participate.
|
| Evaluation | Compare the temperature measurement to baseline data, normal range for age of client, and client’s previous temperatures. Time of day and any additional influencing factors and other vital signs should be analyzed with the body temperature. Appropriate follow-up such as notifying the primary care provider if a temperature is outside of a specific range or is not responding to interventions, giving a medication, or altering the client’s environment. This includes teaching the client how to lower an elevated temperature through actions such as increasing fluid intake, coughing and deep breathing, cool compresses, or removing heavy coverings. Interventions for hypothermia include intake of warm fluids and use of warm or electric blankets. |
Temperature Across the Lifespan
- In Infants, temperature is extremely labile due to thermal dysregulation; the hypothalamus is not yet equipped with regulating body temperature.
- The axillary site is preferred; the arm is held against the chest during assessment. The axilla are not as accurate as other routes, but is safe and non-invasive.
- The tympanic route can be used— fast and convenient. The infant is positioned supine and the head is stabilized. The pinna is pulled straight back and slightly downward for children 3 years old and younger, and upward for those older than 3 years old. The probe is directed anteriorly slightly and advanced until the canal is sealed, but not touching the tympanic membrane. This route is avoided with on-going ear infections.
- The rectal route is the least desirable.
- In Children:
- The tympanic or temporal artery sites are preferred. For tympanic route utilization, the same contraindications are in infants is applied. The child is positioned on the adult’s lap and the head is held gently against the adult for support. The pinna is pulled straight back and upward for children over age 3.
- The oral route may be used, but only non-breakable, electronic thermometers are recommended.
- The rectal route places the child prone on the parent’s lap, or side-lying with the knees flexed. The probe is inserted by 1 inch into the rectum.
- In Older Adults:
- Temperatures tend to be lower, and easily affected by environmental and internal temperature changes. They are at risk of both hypothermia and hyperthermia. The inability of the older adult body to generate or maintain heat can cause their temperature to fail as a measure of seriousness of the pathology of a disease (e.g., pneumonia may only manifest a slight temperature elevation). Alternative assessments should also be used.
- Cerumen impaction may occur and affect the tympanic route.
- Hemorrhoids are also more common in older adults; assessment is required prior to the use of rectal thermometers.