References:
- Kozier & Erb’s Fundamentals of Nursing: Concepts, Process, and Practice, 11th Edition, ISBN 9780135428733, by Audrey Berman, Shirlee J. Snyder, and Geralyn Frandsen (Ch. 28, pp. 532–569)
The pulse is a wave of blood created by contraction of the left ventricle of the heart. Generally, the pulse wave represents the stroke volume output or the amount of blood that enters the arteries with each ventricular contraction. The following are some terms related to pulse:
- Compliance: the ability of arteries to distend (stretch) when pressure is applied by a heart beat, and rebound when the pressure is released.
- Cardiac Output: the amount of blood sent through the body in one minute. This is equal to the stroke volume multiplied by the heart rate. In a resting adult, the heart pumps about 5 liters of blood each minute.
- Stroke Volume: the amount of blood sent through the body with each contraction of the heart.
- Peripheral Pulses: pulses located away from the heart e.g. the foot or wrist.
- Apical (Central) Pulse: the pulse obtained from the apex of the heart, referred to as the point of maximal impulse (PMI)
- Heart Rate: the amount of contractions performed by the heart in one minute.
Factors Affecting the Pulse
- Age: similar to temperature, pulse decreases as age increases.
- Sex: after puberty, the male pulse rate becomes slightly lower than the female pulse rate.
- Exercise: the pulse rate increases with activity depending on cardiac size, strength and efficiency; athletes will experience a slower rate of increase during exercise than the average individual.
- Fever: an elevated body temperature causes vasodilation, which lowers blood pressure, which causes an increased heart rate. A fever also increases metabolic rate, which also contributes to an accelerated pulse.
- Medications: medications that have chronotropic, inotropic, or domotropic effects can increase or decrease pulse rate, strength, and conductivity respectively.
- Hypovolemia or Dehydration: loss of fluid from the vascular system increases the pulse rate as the heart attempts to increase blood pressure.
- Stress: sympathetic nervous stimulation increases the overall activity of the heart in both rate and force. Causes of stress include fear, anxiety, and acute pain.
- Position: dependent positioning (sitting or standing) decreases venous blood return and subsequent reduction in blood pressure, increasing the heart rate.
- Pathology: certain diseases such as heart conditions or those that impair oxygenation can alter the resting pulse rate.
| Age | Pulse Average | Respiration Average |
|---|---|---|
| Newborn | 130 (80-180) | 35 (30-60) |
| 1 year | 120 (80-140) | 30 (20-40) |
| 5-8 years | 100 (75-120) | 20 (15-25) |
| 10 years | 70 (50-90) | 19 (15-25) |
| Teen | 75 (50-90) | 18 (15-20) |
| Adult | 80 (60-100) | 16 (12-20) |
| Older Adult | 70 (60-100) | 16 (15-20) |
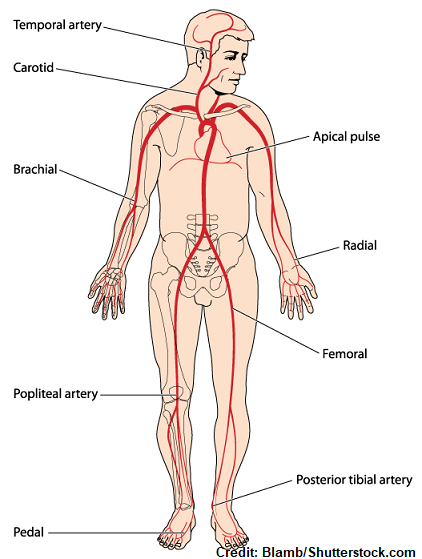
Pulse Sites
- Temporal, where the temporal artery passes over the temporal bone of the head. It is above and to the side (superior and lateral) of the eye.
- Carotid, at the side of the neck where the carotid artery between the trachea and the sternocleidomastoid muscle.
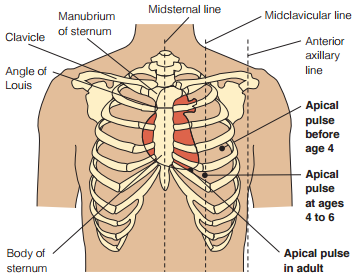
- Apical, at the apex of the heart. In an adult, this is located on the left side of the chest about 8 cm (3 in.) to the left of the sternum (breastbone) at the fifth intercostal space. This may be further left in cardiomegaly. The location of the apical pulse also changes during childhood, illustrated below.
- Brachial, at the inner aspect of the biceps muscle of the arm or medially in the antecubital space.
- Radial, where the radial artery runs along the radial bone, on the thumb side of the inner aspect of the wrist.
- Femoral, where the femoral artery passes alongside the inguinal ligament.
- Popliteal, where the popliteal artery passes behind the knee.
- Posterior tibial, on the medial surface of the ankle where the posterior tibial artery passes behind the medial malleolus.
- Dorsalis pedis, where the dorsalis pedis artery passes over the bones of the foot, on an imaginary line drawn from the middle of the ankle to the space between the big and second toes.
| Pulse Site | Location | Reasons for Use |
|---|---|---|
| Radial | Thumb side, inner aspect of the wrist | Readily accessible |
| Temporal | Temporal bone, supralateral to the eye | Used when radial pulse is not accessible |
| Carotid | Between the trachea and the sternocleidomastoid muscle. | Used during cardiac arrest or shock in adults Used to determine circulation to the brain |
| Apical | 8 centimeters left of the sternum at the fifth intercostal space* | Routinely used for infants and children up to 3 years of age. Used to determine discrepancies with radial nurse Used in conjunction with some medications |
| Brachial | Inner aspect of the biceps muscle; medially in the antecubital space | Used to measure blood pressure Used during cardiac arrest for infants |
| Femoral | Along the inguinal ligament | Used in cases of cardiac arrest or shock Used to determine circulation to a leg |
| Popliteal | Behind the knee | Used to determine circulation to the lower leg |
| Posterior tibial | Medial surface o the ankle behind the medial malleolus | Used to determine circulation to the foot |
| Dorsalis pedis | From the middle of the ankle to the space between the big and second toes | Used to determine circulation to the foot |
Assessing the Pulse
A pulse is commonly asses through palpation or auscultation.
- Palpation: middle three fingers placed on the pulse site; used for all sites except the apex of the heart. The fingers of the hand should apply moderate pressure; too light and a pulse may not be palpated, while too firm and the pulse may be obliterated.
- Auscultation: a stethoscope is used for assessing apical pulses. In difficult-to-assess pulses (usable in noisy environments), a doppler ultrasound stethoscope may be used.
Be Aware
The nurse should be aware of the following:
- Any medication that could affect the heart rate.
- Whether the client has been physically active. If so, wait 10 to 15 minutes until the client has rested and the pulse has slowed to its usual rate.
- Any baseline data about the normal heart rate for the client. For example, a physically fit athlete may have a resting heart rate below 60 beats/min.
- Whether the client should assume a particular position (e.g., sitting). In some clients, the rate changes with the position because of changes in blood flow volume and autonomic nervous system activity.
The pulse can be assessed according to rate, rhythm, volume, arterial wall elasticity, and presence or absence of bilateral equality.
- Rate: >100 beats/min is considered tachycardia and <60 beats/min is considered bradycardia. In either case, if this is observed, the nurse must obtain the apical pulse.
- Rhythm: the pattern and intervals of the beats. In a normal pulse, beats are spaced in equal time intervals. A pulse with an irregular rhythm is referred to as a dysrhythmia or arrhythmia. These appear as random, irregular beats or a predictable pattern of irregular beats (“regularly irregular”). The apical pulse should be assessed if any abnormality is observed, and an ECG is necessary to define the dysrhythmia further.
- Pulse Volume: “strength” or “amplitude”. The force of the blood with each beat, ranging from absent to bounding. Absent pulses are weak and easily obliterated even without moderate pressure, while bounding pulses are strong and difficult to obliterate.
| Grade | Pulse Characteristic |
|---|---|
| 0 | Absent; non-palpable pulses |
| 1 | Weak, thready pulses |
| 2 | Normal; easily distinguishable pulses |
| 3 | Strong pulses; bounding |
- Arterial Wall Elasticity: upon palpation, healthy, normal arteries feel straight, smooth, soft, and pliable. The loss of elasticity often appear as a tortuous (twisted) and irregular artery upon palpation.
- Bilateral Equality: checking for perfusion to a peripheral pulse should also warrant the assessment of the corresponding pulse on the other side of the body. The second assessment gives the nurse data with which to compare the pulses. In assessing perfusion, the nurse starts at the most distal pulse site (e.g., dorsalis pedis) and makes their way up the extremity until a pulse is found.
Patient-Centered Care
Clients can be provided guidance in relation to pulse assessment at home.
- Teach the client to monitor the pulse prior to taking medications that affect the heart rate. The client should know to report any notable changes in heart rate or rhythm.
- Inform the client about activities known to significantly affect pulse rate such as emotional stress, exercise, ingesting caffeine, and sleep. If clients are sensitive to pulse rate changes, they should consider the modification of these activities to stabilize the pulse.
- Lengthy monitoring may use a Holter monitor, an ambulatory recorder usable for 24 hours or longer. Other cardiac event monitors also exist, such as those activated during periods of exacerbation.
Pulse Deficit
A pulse deficit is a difference between apical and peripheral pulses. This warrants an apical-radial pulse assessment.
Pulse Assessment Procedure
Peripheral pulses are obtained for purposes such as:
- To establish baseline data for subsequent evaluation.
- To identify whether the pulse rate is within the normal range.
- To determine the pulse volume and whether the pulse rhythm is regular.
- To determine the equality of corresponding peripheral pulses on each side of the body.
- To monitor and assess changes in the client’s health status.
- To monitor clients at risk for pulse alterations.
- To evaluate blood perfusion to the extremities.
| Phase | Nursing Activities |
|---|---|
| Assessment | Assess clinical signs of cardiovascular alterations, factors that alter pulse rates, and which sites are most appropriate based on the purpose of the assessment. - Signs of cardiovascular alterations: dyspnea, fatigue, pallor, cyanosis, palpitations, syncope, or impaired peripheral tissue perfusion. |
| Planning | Assign: radial or brachial pulse assessment may be assigned to APs or family members or caregivers in nonhospital settings. The nurse bears responsibility for abnormal pulses (rate or rhythm), appropriate action after confirmation, and use of techniques for sites other than radial or brachial artery and Doppler ultrasound devices. Equipment: clock, timer, or watch with a sweep second hand or digital seconds indicator. If a DUS is being used, the probe, headset (for some models), transmission gel, and tissues or wipes are prepared. |
| Implementation | Make sure all gathered equipment are functioning normally. Prior to performing the procedure, the nurse must introduce themselves and verify the client’s identity using agency protocol. Explanation of the nurse’s purpose, the procedure, and how the patient will participate.
|
| Evaluation | Compare the pulse rate, rhythm, and volume to recent, baseline, or usual range for the age of the client and other vital signs or health status. In assessing peripheral pulses, equality, rate, and volume are all assessed in corresponding extremities. Appropriate follow-up is conducted for notifying the primary care provider of any abnormalities or after the administration of medication. |
Assessing an Apical Pulse
The apical pulse is obtained for purposes such as:
- To obtain the heart rate of an adult with an irregular peripheral pulse.
- To establish baseline data for subsequent evaluation.
- To determine normalcy and regularity of the cardiac rate.
- To monitor clients with cardiac, pulmonary, or renal disease and those receiving medications to improve heart action.
| Phase | Nursing Activities |
|---|---|
| Assessment | Assess clinical signs of cardiovascular alterations, and factors that may alter pulse rate. - Signs of cardiovascular alterations: dyspnea, fatigue, pallor, cyanosis, palpitations, syncope, or impaired peripheral tissue perfusion. |
| Planning | Assign: apical pulse assessment is not performed by APs. Equipment: clock, timer, or watch with a sweep second hand or digital seconds indicator; stethoscope; and antiseptic wipes. If a DUS is being used, the probe, headset (for some models), transmission gel, and tissues or wipes are prepared. |
| Implementation | Make sure all gathered equipment are functioning normally. Prior to performing the procedure, the nurse must introduce themselves and verify the client’s identity using agency protocol. Explanation of the nurse’s purpose, the procedure, and how the patient will participate.
|
| Evaluation | Compare the pulse rate, rhythm, and volume to recent, baseline, or usual range for the age of the client and other vital signs or health status. Report to the primary care provider and other relevant members of the healthcare team any abnormal findings such as irregular rhythm, reduced ability to hear the heartbeat, pallor, cyanosis, dyspnea, tachycardia, or bradycardia. Appropriate follow-up is conducted, such as administering medication ordered based on apical heart rate. |
Assessing an Apical-Radial Pulse
In cases of suspected peripheral circulation inadequacy or a pulse deficit, an apical-radial pulse is obtained. This involves obtaining apical and radial rates simultaneously to determine abnormalities such as a pulse too weak to be felt at the peripheral pulses, or the presence of vascular disease that prevents impulses from being transmitted. A discrepancy in apical pulse rate and peripheral pulse rate is called a pulse deficit and must be reported immediately. This technique can be performed by one or two nurses.
| Phase | Nursing Activities |
|---|---|
| Assessment | Assess clinical signs of hypovolemic shock (hypotension, pallor, cyanosis, and cold, clammy skin). |
| Planning | Assign: apical-radial pulse assessment is not performed by APs. Equipment: clock, timer, or watch with a sweep second hand or digital seconds indicator; stethoscope; and antiseptic wipes. |
| Implementation | If using the two-nurse technique, ensure that the second nurse is available. Prior to performing the procedure, the nurse must introduce themselves and verify the client’s identity using agency protocol. Explanation of the nurse’s purpose, the procedure, and how the patient will participate.
|
| Evaluation | Compare the pulse rate, rhythm, and volume to recent, baseline, or usual range for the age of the client and other vital signs or health status. Report any changes from previous measurements or any discrepancy between the two pulse rates. |
Pulse Across the Lifespan
- Newborns may have physiologic (expected) heart murmurs. These reflect functional incomplete closure of fetal heart structures (ductus arteriosus or foramen ovale).
- Infants: apical pulse is used up to 2 to 3 years old to establish baseline data, normalcy, and regularity of the rhythm. The infant is placed supine while the infant is comfortable and rested; this necessitates apical pulse assessment ahead of other uncomfortable procedures to avoid artificial elevation of pulse findings.
- Children: the child is placed in the adult’s arms or close to the adult. This may decrease anxiety and yield more accurate results. In apical pulses, children are placed supine or sitting like adults. Prior to assessment, play-based demonstration (with a stuffed animal or doll) may be done along with allowing the child to handle the stethoscope before beginning the procedure. This promotes cooperation and decreases anxiety.
- Older Adults: severe hand or arm tremors may make radial pulse assessment difficult. Peripheral pulses become less reliable in old age due to decreased cardiac output, sclerotic changes, and dysrhythmias. An apical pulse is increasingly more preferred over peripheral pulses. Contrastingly, this weakness of the peripheral pulse warrants assessment of pedal pulses for regularity, volume, and symmetry. This age group also takes a longer period to return to their baseline values after activity.