References:
- Kozier & Erb’s Fundamentals of Nursing: Concepts, Process, and Practice, 11th Edition, ISBN 9780135428733, by Audrey Berman, Shirlee J. Snyder, and Geralyn Frandsen (Ch. 28, pp. 532–569)
Arterial blood pressure is the pressure placed on the blood vessels by the heart during its systolic (contractile) and diastolic (relaxed) phases.
- Systolic Pressure: the blood pressure at the moment of ejection/during contraction of the heart.
- Diastolic Pressure: the blood pressure at the moment of filling/relaxation of the heart.
- Pulse Pressure: the pressure difference between systolic and diastolic () that indicates the amount of pressure produced by a contraction of the heart, which is often used to reflect fluid status of an individual. It normally sits around 40 mm Hg and ranges from 30 to 50 mm Hg. A consistently heightened pulse pressure occurs in arteriosclerosis, and a low pulse pressure occurs in conditions such as severe heart failure.
- Mean Arterial Pressure: the actual pressure actually delivered to the body’s organs. There are a few ways to calculate this value. Try to check which one is the easiest to remember or to perform.
- (1) Calculating MAP:
- (2) Calculating MAP:
- (3) Calculating MAP:
Normal Blood Pressure Ranges
The American Heart Association (AHA) applies classifications of hypertension with the following criteria:
Category Systolic Blood Pressure Diastolic Blood Pressure Normal <120 mm Hg and <80 mm Hg Elevated (Prehypertension) 120-129 mm Hg and <80 mm Hg Hypertension I 130-139 mm Hg or 80-89 mm Hg Hypertension II 140+ mm Hg or 90+ mm Hg Hypertensive Crisis 180+ mm Hg and/or 120+ mm Hg
Determinants and Factors Affecting Blood Pressure
Determinants are the aspects that make up the pressure forces measured in blood pressure.
- Pumping Action of the Heart: weaker pumping equates to lower cardiac output, and decreased blood pressure. The opposite is also true.
- Peripheral Vascular Resistance: vascular capacity (internal diameter of capillaries and arterioles), arterial compliance, and blood viscosity affect peripheral vascular resistance— the pressure the blood has to fight against to flow. Increased vasoconstriction (such as in smoking), increased viscosity, or arteriosclerosis are all causes for increasing peripheral vascular resistance, increasing blood pressure.
- Blood Volume: blood volume is proportional to blood pressure. In cases of fluid overload from rapid IV infusion or pregnancy, blood pressure increases.
- Blood Viscosity: thick blood (hemoconcentration; Hct > 60%-65%) makes blood more resistant to flow, necessitating an increased blood pressure.
Factors are extraneous conditions that contribute to blood pressure, but is not directly a constituent of blood pressure.
- Age: newborns have a systolic pressure of about 75 mm Hg, which rises with age, reaching its peak during puberty, then declines somewhat. In older adults, arteriosclerosis elevates systolic and even diastolic pressure.
- Exercise: physical activity increases cardiac output and hence blood pressure. For reliable assessment of resting blood pressure, wait 20 to 30 minutes following exercise.
- Stress: stimulation of the sympathetic nervous system increases cardiac output and vasoconstriction of the arterioles, thus increasing the blood pressure reading; however, severe pain can decrease blood pressure greatly by inhibiting the vasomotor center and producing vasodilation.
- Race: African American individuals older than 35 years tend to have higher blood pressures than other races of the same age.
- Sex: females usually have lower blood pressures than males of the same age after puberty, raising after menopause. This difference is thought to be due to hormonal variations. After the age of 65, the rate of high blood pressure is higher in women than it is in men of the same age.
- Medications: caffeine and many other medications may increase or decrease the blood pressure.
- Obesity: childhood and adult obesity is a major predisposing factor for hypertension.
- Diurnal Variations: similar to temperature, blood pressure is the lowest in early morning and peaks in the late afternoon or early evening.
- Medical Conditions: any condition affecting cardiac output, blood volume, blood viscosity, or compliance of the arteries has a direct effect on the blood pressure.
- Temperature: increased temperature from a fever increases metabolic rate, which increases blood pressure. However, in external heat vasodilation occurs which decreases blood pressure. Inversely, cold will cause vasoconstriction and increase blood pressure.
Alterations in Blood Pressure
Hypertension is a persistent elevation of blood pressure. A single elevated blood pressure reading indicates the need for reassessment— a diagnosis is only made after two elevated measurements measured at different times. In most cases, hypertension is asymptomatic and is often a contributing factor to myocardial infarctions (heart attacks).
- Primary Hypertension: the most common form of hypertension, whose cause is unknown.
- Secondary Hypertension: hypertension resultant of known causes.
Factors associated with hypertension include thickening of the arterial walls, which reduces the size of the arterial lumen, and inelasticity of the arteries, as well as lifestyle factors as cigarette smoking, obesity, heavy alcohol consumption, lack of physical exercise, high blood cholesterol levels, and continued exposure to stress.
Hypotension is a blood pressure that is below normal, that is, a systolic reading consistently between 85 and 110 mmHg in an adult whose normal pressure is higher than this. Orthostatic Hypotension (postural hypotension) is a blood pressure that decreases when the client changes from a supine to a sitting or standing position, often the result of peripheral vasodilation in which the blood leaves the central body organs, especially the brain, and moves to the periphery, often causing the client to feel faint.
Assessing for Orthostatic Hypotension
- Place the client in a supine position for at least five minutes, then record the client’s pulse and blood pressure.
- Assist the client to a seated or standing position. Immediately recheck the pulse and blood pressure in the same sites as previously, then again in three minutes.
- Record the results. A drop in blood pressure of 20 mmHg systolic or 10 mmHg diastolic or an increase of 20 beats/min indicates orthostatic hypotension.
Hypotension may be caused by analgesics such as meperidine hydrochloride (Demerol), bleeding, severe burns, and dehydration. It is important to monitor hypotensive clients carefully to prevent falls.
Assessing Blood Pressure
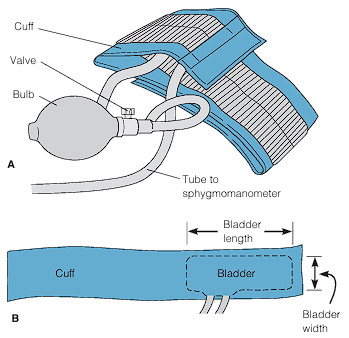
Manual blood pressure management is performed with a blood pressure cuff, a sphygmomanometer, and a stethoscope. The cuff consists of a bag (bladder) that is inflated with air. To the bladder, there are two tubes that connect the pump (bulb) and the sphygmomanometer, which displays the pressure in the bag. There are two types of sphygmomanometers: aneroid, which is a gauge with a calibrated dial with a needle that points to the calibrations; and digital, which eliminates the need to auscultate the client’s systolic and diastolic blood pressures through a stethoscope. Doppler ultrasound stethoscopes are also used to assess blood pressure, especially useful for infants, obese clients, and clients in shock where blood pressure sounds are difficult to hear.
Choosing Blood Pressure Cuff Sizes
- Bladder Width: 40% of the arm circumference, or 20% wider than the diameter. Erroneously high readings are found if the width is too narrow, and vice versa.
- Bladder Length: at least two-thirds of the limb’s circumference.
The most common site for blood pressure assessment is the upper arm, but it may be measured from the forearm, wrist, or thigh in case of contraindications. These contraindications include:
- The site for assessment is injured or diseased.
- The limb for assessment has a cast or bulky bandage.
- The client has had surgical removal of breast or axillary (or inguinal) lymph nodes on that side.
- The client has an IV infusion or blood transfusion in that limb.
- The client has an arteriovenous fistula (e.g., for renal dialysis) in that limb.
Blood pressure may be measured directly or indirectly. Direct (invasive) monitoring involves the insertion of a catheter into the brachial, radial, or femoral artery. Arterial pressure is represented as wavelike forms displayed on a monitor. With correct placement, this pressure reading provides very highly accuracy. As nurses, most measurements will be done noninvasively; indirectly. This may be done with two techniques:
- Auscultatory Method: the use of a stethoscope to listen for Korotkoff sounds, particularly phase 1 and phase 5, to determine the systolic and diastolic blood pressures respectively.
- Korotkoff Phase 1: “A sharp tapping”, which gradually becomes more intense.
- Korotkoff Phase 2: “A swishing or whooshing sound”.
- Korotkoff Phase 3: “A thump softer than the tapping in phase 1”, which sounds crisper and more intense but again softer than in phase 1.
- Korotkoff Phase 4: “A softer blowing muffled sound that fades”. In some institutions, this may be considered the “first diastolic measurement”.
- Korotkoff Phase 5: “Silence”. The pressure level when the last sound is heard. This is the diastolic pressure commonly recorded.
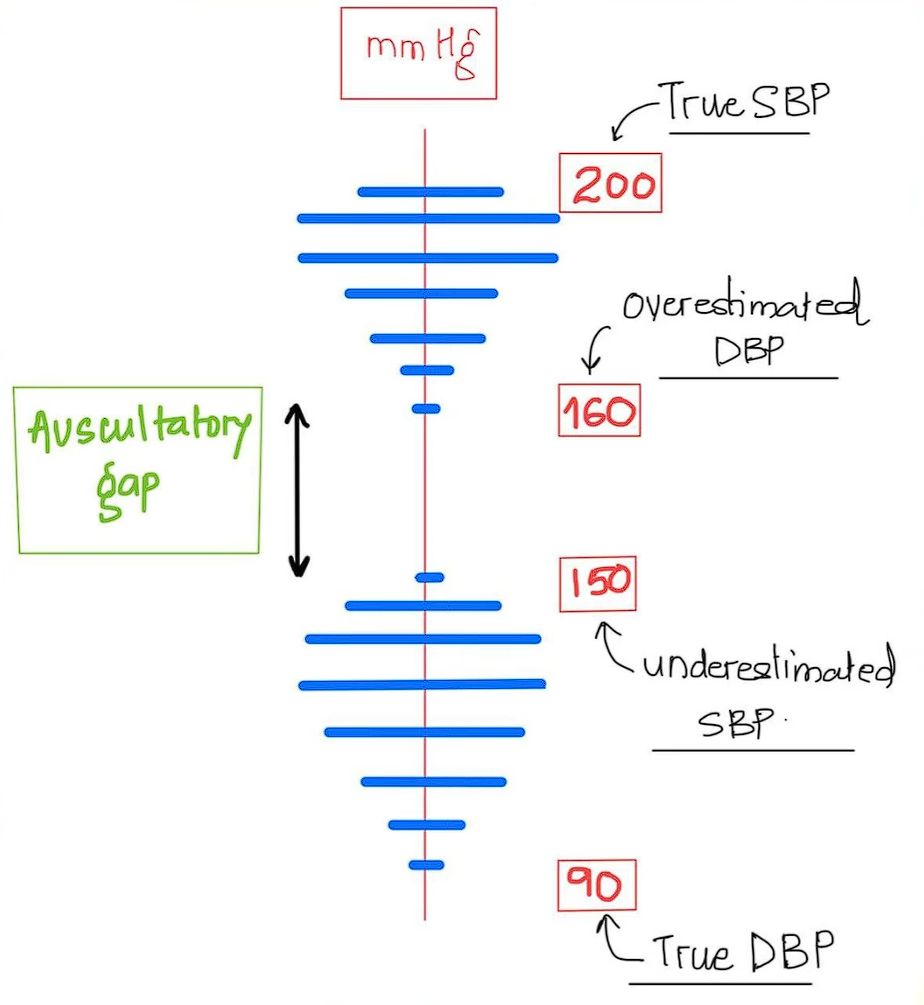
Auscultatory Gap
The auscultatory gap is a phenomenon where phase 1 to phase 3 of the Korotkoff sounds become difficult to hear and appear as silence, even when the pulse is still palpable. This results in an underestimated systolic blood pressure and an overestimated diastolic blood pressure. This phenomenon is demonstrated and explained by Dr. Sourya Acharya (also the source of the following image).
- Palpatory Method: this method is less common, but is used when Korotkoff sounds cannot be heard and electronic equipment to amplify the sounds is not available, or to prevent misdirection from the presence of an auscultatory gap. Similar to the auscultatory method, the nurse uses light to moderate pressure to palpate the pulsations of the artery as the pressure in the cuff is released. The first pulsation felt after releasing the pressure in the cuff is the systolic pressure. A single whiplike vibration, felt in addition to the pulsations, identifies the point at which the pressure in the cuff nears the diastolic pressure. This vibration is no longer felt below the diastolic pressure.
Preparation
Patients must rest approximately 15 minutes after activity for an accurate blood pressure reading. For those who are caffeinated or have smoked, a 30 minute rest period is given in order to obtain an accurate reading. When reading, the patient is seated if possible.
The nurse inflates the cuff one to two inches above the brachial artery (if being taken at the popliteal fossa) up to 30 to 50 mm Hg above the pressure where the pulse becomes obliterated. Once deflated slowly (2 to 3 mm Hg/s), there are five Korotkoff sounds that the nurse hears:
- Korotkoff 1: the first tap or thud indicating the return of blood flow, representing the systolic pressure.
- Korotkoff 2: a swishing or whooshing
- Korotkoff 3: a thumping sound
- Korotkoff 4: a blowing sound
- Korotkoff 5: The following silence. The point at which the diastolic has returned, and is recorded as the diastolic pressure.
Mistakes in Blood Pressure Taking
Error Effect Bladder cuff too narrow Erroneously high Bladder cuff too wide Erroneously low Arm unsupported Erroneously high Insufficient rest before the assessment Erroneously high Repeating assessment too quickly Erroneously high systolic or low diastolic readings Cuff wrapped too loosely or unevenly Erroneously high Deflating cuff too quickly Erroneously low systolic and high diastolic readings Deflating cuff too slowly Erroneously high diastolic readings Failure to use the same arm consistently Inconsistent measurements Arm above level of the heart Erroneously low Assessing immediately after a meal or while client smokes or has pain Erroneously high Failure to identify auscultatory gap Erroneously low systolic pressure and erroneously low diastolic pressure
Blood Pressure Assessment Procedure
Assessing respirations is done to:
- Establish baseline measurement of arterial blood pressure for subsequent evaluation.
- Determine the client’s hemodynamic status (e.g., cardiac output: stroke volume of the heart and blood vessel resistance)
- Identify and monitor changes in blood pressure resulting from a disease process or medical therapy
| Phase | Nursing Activities |
|---|---|
| Assessment | Assess for signs and symptoms of hypertension (e.g., headache, ringing in the ears, flushing of face, nosebleeds, fatigue), of hypotension (e.g., tachycardia, dizziness, mental confusion, restlessness, cool and clammy skin, pale or cyanotic skin) Determine any factors that could change blood pressure such as recent activity, emotional stress, pain, and time the client last smoked or ingested caffeine. In cases of activity or caffeine intake, the nurse must wait for 30 minutes in order to obtain a reliable reading. |
| Planning | Assign: blood pressure measurement may be assigned to AP. The nurse interprets abnormal blood pressure readings and determines appropriate responses. Equipment: stethoscope or DUS, blood pressure cuff of the appropriate size, and sphymomanometer. |
| Implementation | Ensure that the equipment is intact and functioning properly. Check for leaks in the tubing between the cuff and the sphygmomanometer. Calibrate as necessary. Ensure that it has been at least 30 minutes since the last ingestion of caffeine or smoking. Prior to performing the procedure, the nurse must introduce themselves and verify the client’s identity using agency protocol. Explanation of the nurse’s purpose, the procedure, and how the patient will participate.
|
| Evaluation | Relate blood pressure to other vital signs, to baseline data, and to health status. If findings are significant different from previous values without obvious reasons, consider possible causes of error. Any significant changes are reported. Abnormal findings that persist over time are also reported:
|
Procedural Variations
- Palpation Method: if a stethoscope is not usable, palpate the radial or brachial pulse sites as the cuff pressure is released. The manometer reading at the point where the pulse reappears is an estimate of systolic value. The manometer reading at the point where the whiplike vibration appears is an estimate of the diastolic pressure.
- Thigh Blood Pressure: - The patient is positioned prone. If contraindicated, the client is positioned supine with the knee slightly flexed. - Expose the thigh, taking care not to expose the client unduly. - Locate the popliteal artery. - Wrap the cuff evenly around the midthigh with the compression bladder over the posterior aspect of the thigh and the bottom edge above the knee. - If this is the client’s initial examination, perform a preliminary palpatory determination of systolic pressure by palpating the popliteal artery. - In adults, the systolic pressure in the popliteal artery is usually 20 to 30 mmHg higher than that in the brachial artery; the diastolic pressure is usually the same.
- Electronic Indirect Blood Pressure Monitoring Device: an automated machine can be given a preset for wait periods, repeated assessments, and averaged assessments while the client is resting quietly, seated in a chair, and alone in the room. This can also be left in place for many hours. The cuff should be removed periodically to check skin condition.
Blood Pressure Across the Lifespan
- Infants:
- A pediatric stethoscope should be used.
- The lower edge of the blood pressure cuff can be closer to the antecubital space of an infant.
- Use the palpation method if auscultation is unsuccessful.
- Arm and thigh pressures are equivalent in children under 1 year of age. (There is a difference of 20 to 30 mmHg in the systolic pressures of the arm and thigh in adults)
- The systolic blood pressure of a newborn averages about 70 mmHg, but is not usually recorded due to technical difficulty except when problems are suspected.
- Children:
- Blood pressure should be measured in all children over 3 years of age and in children less than 3 years of age with certain medical conditions.
- All steps of the procedures and what it will feel like should be explained. A demonstration on a doll can be done.
- Use the palpation technique for children under 3 years old.
- Cuff bladder width should be 40% and length should be 80% to 100% of the arm circumference.
- Diastolic pressure is considered to be based on Korotkoff sounds phase 4 rather than phase 5 in children.
- Arm and thigh pressures differ by about 10 mmHg.
- In children, normal blood pressure can be determined quickly with the formula .
- Older Adults:
- Skin may become fragile. Cuff pressure should not be kept high for any longer than necessary.
- Clients may be taking antihypertensives. Determine when the last dose was taken, if any.
- Medications that cause vasodilation and also the loss of baroreceptor efficiency in older adults place them at an increased risk for having orthostatic hypotension. Assess for orthostatic hypotension.
- If the client has arm contractures, assess the blood pressure by palpation, with the arm in a relaxed position. A wrist or thigh reading may be taken if this is not possible.