References:
- Kozier & Erb’s Fundamentals of Nursing: Concepts, Process, and Practice, 11th Edition, ISBN 9780135428733, by Audrey Berman, Shirlee J. Snyder, and Geralyn Frandsen (Ch. 29, pp. 579–587)
The integument includes the skin, hair, and nails. The examination begins with a generalized inspection using a good source of lighting, preferably indirect natural daylight.
Skin
Skin: inspection (sight, smell) and palpation.
- Pungent body odor related to poor hygiene, hyperhidrosis, or bromhidrosis.
- Pallor: paleness due to inadequate circulating blood. This is most readily seen in areas of least pigmentation such as the conjunctiva, oral mucous membranes, nail beds, palms of the hand, and soles of the feet. In dark/black skin, it appears ashen gray. In brown skin, it may appear as a yellowish brown tinge.
- Cyanosis: a bluish tinge most evident in the nail beds, lips, and buccal mucosa. The palpebral conjunctiva, palms, and soles are used to determine the presence of cyanosis in dark-skinned clients.
- Jaundice: a yellowish tinge commonly first evident in the sclera of the eyes and then in the mucous membranes and the skin. Take care not to confuse the normal yellow tinged sclera that may be present in some dark skinned clients— if suspected, observe for jaundice at the posterior hard palate in clients to verify the presence of jaundice.
- Erythema: skin redness associated with a variety of rashes and other conditions.
- Hyper- and hypopigmentation: changes in the distribution of melanin or in the function of the melanocytes in the epidermis. Examples include birthmarks or vitiligo. Albinism is the complete or partial lack of melanin in the skin, hair, and eyes. It may also point to problems, such as edema or a localized infection.
- Edema: the presence of excess interstitial fluid. It appears swollen, shiny, and taut and tends to blanch the skin color or, if accompanied by inflammation, may redden the skin. Generalized edema (anasarca) is most often an indication of impaired venous circulation and in some cases reflect cardiac dysfunction or venous abnormalities.
- Skin lesions: alterations in a client’s normal skin appearance either as primary lesions (due to changes in the external or internal environment of the skin) or secondary lesions that result from chronicity, trauma, or infection of the primary lesion.
- Describe lesions in terms of location, distribution, configuration, color, shape, size, firmness, texture, and characteristics of individual lesions.
| Lesion | Description |
|---|---|
| Primary, Flat | |
| Macule | 1 mm to 1 cm. Flat, unelevated change in color. Circumscribed. |
| Patch | >1 cm. Flat, unelevated change in color. May be irregular. |
| Primary, Elevated | |
| Papule | <1 cm. Circumscribed, solid elevation of skin |
| Plaque | >1 cm. Solid elevation of skin. |
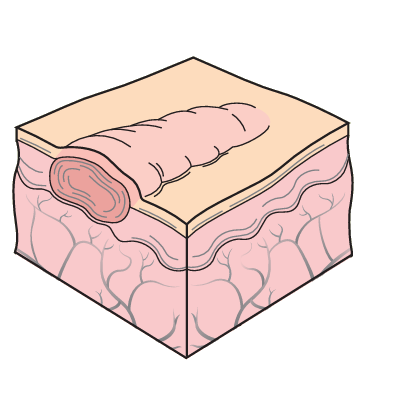
| Nodule | 0.5–2 cm. Solid, hard mass that extends deeper into the dermis than a papule. Borders are circumscribed. |
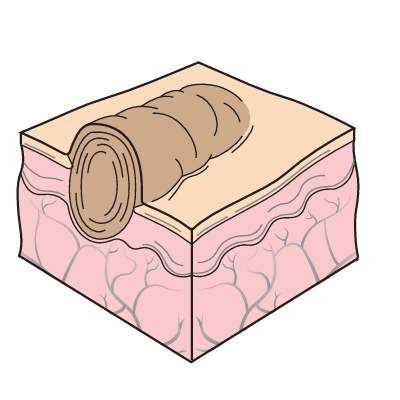
| Tumor | >2 cm. Solid, hard mass that extends deeper into the dermis than a papule. Borders may not be easily distinguishable. |
| Primary, Fluid-filled | |
| Pustule | Varying sizes. Vesicle or bulla filled with pus. |
| Vesicle | <0.5 cm. Circumscribed, round or oral, thin translucent mass filled with serous fluid or blood. |
| Bulla | >0.5 cm. Circumscribed, round or oral, thin translucent mass filled with serous fluid or blood. |
| Cyst | >1 cm. Encapsulated, fluid-filled or semisolid mass arising from the subcutaneous tissue or dermis. |
| Wheal | Varying sizes. Reddened, localized collection of edema fluid; irregular in shape |
| Secondary | |
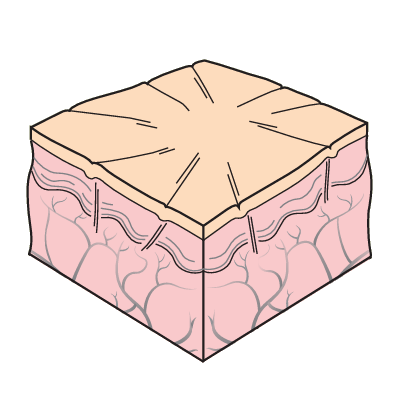
| Atrophy | Translucent, dry, paper-like, sometimes wrinkled skin surface resulting from thinning or wasting of the skin due to loss of collagen and elastin. |
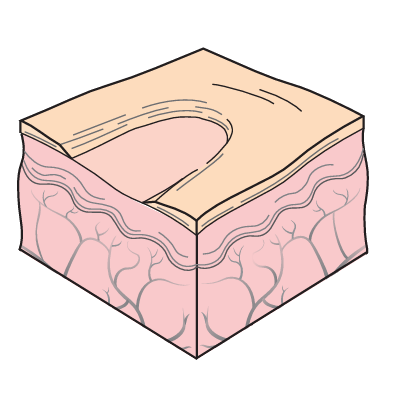
| Erosion | Wearing away of the superficial epidermis causing a moist, shallow depression. |
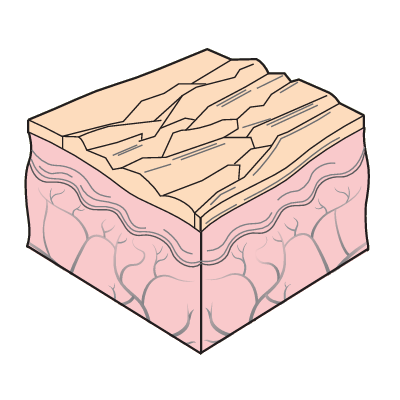
| Lichenification | Rough, thickened, hardened area of epidermis resulting from chronic irritation such as scratching or rubbing. |
| Scales | Shedding flakes of greasy, keratinized skin tissue. |
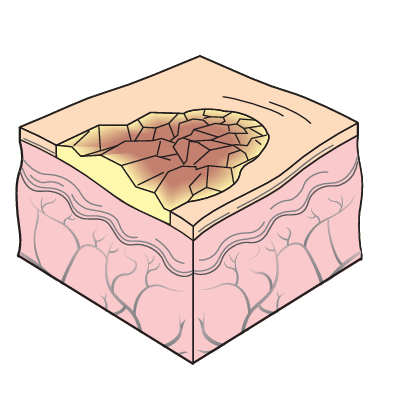
| Crust | Dry blood, serum, or pus left on the skin surface when vesicles or pustules burst. Can be red-brown, orange, or yellow. If large crusts adhere to the skin, they are called scabs. |
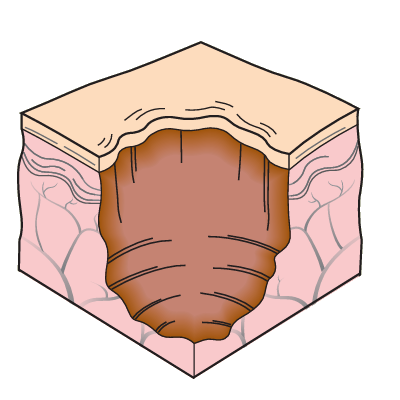
| Ulcer | Deep, irregularly shaped area of skin loss extending into the dermis or subcutaneous tissue. May bleed. May leave scar. |
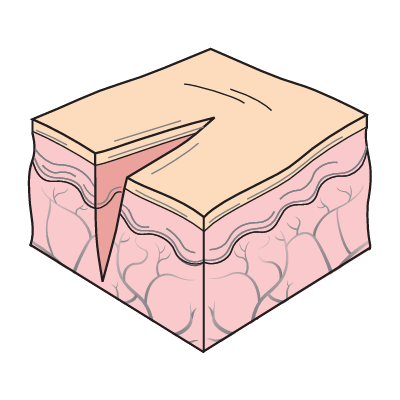
| Fissure | Linear crack with sharp edges, extending into the dermis. |
| Scar | Flat, irregular area of connective tissue left after a lesion or wound has healed. Color may appear red or purple for new scars, and silvery and white for old scars. |
| Keloid | Elevated, irregular, darkened area of excess scar tissue caused by excessive collagen formation during healing, extending beyond the site of the original injury. |
| Excoriation | Linear erosion |
The following images are all from Kozier & Erb's Fundamentals of Nursing Book!









Hair
Assessing a client’s hair includes inspecting the hair, considering developmental changes and ethnic differences, and determining the individual’s hair care practices and factors influencing them. Much of the information about hair can be obtained by questioning the client.
- Hair is normally resilient and evenly distributed.
- Faded or even reddish or bleached dry, coarse hair can result from severe protein deficiency (kwashiorkor).
- Thin and brittle hair can appear in hypothyroidism.
- Alopecia can occur in some therapies.
Nails
Inspect for shape, angle between the fingernail and nail bed, nail texture, nail bed color, and the intactness of tissues around the nails. Nails are normally colorless and has a convex curve; the angle between the nail bed and fingernail is 160 degrees.
- Koilonychia: spoon-shaped nails, seen in patients with iron-deficiency anemia.
- Clubbing: the angle of the nail and nail bed increases to 180 degrees or greater, potentially caused by a long-term lack of oxygen.
- Thick Nails: excessively thick nails can be seen in older adults, due to poor circulation, or in relation to a chronic fungal infection.
- Thin Nails: grooves or furrows due to prolonged iron-deficiency anemia can make the nail appear thin.
- Beau’s Lines are horizontal depressions in the nail that can result from injury or severe illness.
- Discolored Nail Beds: nails are highly vascular, a characteristic that accounts for its color. Cyanosis and pallor are easily observed through the nail beds.
- Onychomycosis (nail fungus) should be referred to a podiatrist or dermatologist for treatment of nail fungus. Symptoms include brittleness, discoloration, thickening, distortion of nail shape, crumbling of the nail, and loosening of the nail.
- Paronychia: inflammation of the tissues surrounding a nail. Inflammation, swelling, and tenderness are usually present.
- Slow Capillary Refill is reflective of perfusion, and is observed with the blanch test— the application of pressure to blanch the nail bed, after which they should quickly turn pink (or their usual color) when pressure is released.