References:
- Kozier & Erb’s Fundamentals of Nursing: Concepts, Process, and Practice, 11th Edition, ISBN 9780135428733, by Audrey Berman, Shirlee J. Snyder, and Geralyn Frandsen (Ch. 29, pp. 588–603)
During assessment of the head, the nurse inspects and palpates simultaneously and also auscultates. The nurse examines the skull, face, eyes, ears, nose, sinuses, mouth, and pharynx.
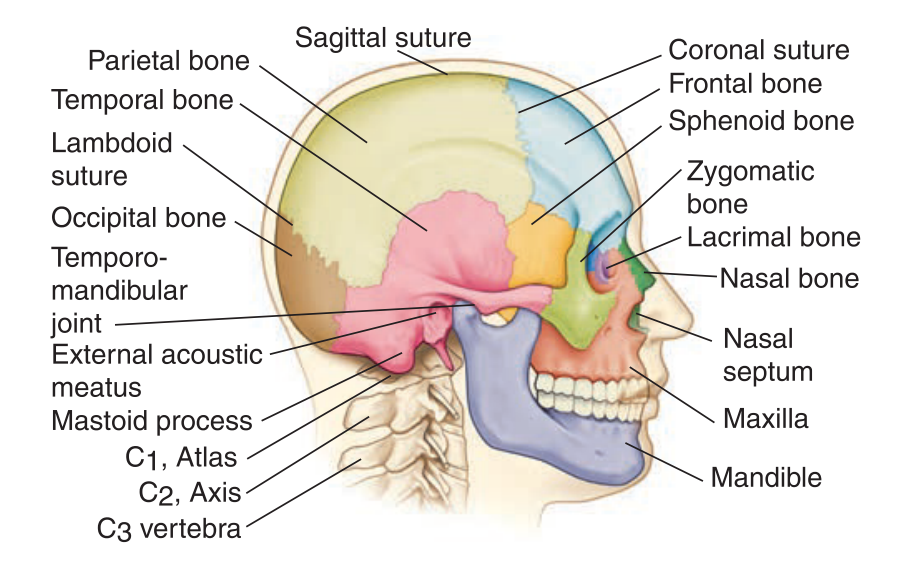
Skull and Face
A normal skull can be of a multitude of forms. Normal head size (“normocephaly”) is determined by being within a two standard deviations on the normal size chart based on age, sex, and race of the client.
- Edema of the Eyelids: kidney or cardiac disease
- Exophthalmos, a protrusion of the eyeballs, is common in hyperthyroidism.
- Dry, puffy face with dry skin and coarse features and thinning of scalp hair and eyebrows: hypothyroidism.
- Moon face (round face with reddened cheeks) can appear in increased adrenal hormone production along with excessive hair growth on the upper lips, chin, and sideburn areas.
- Sunken eyes, cheeks, and temples can be observed in prolonged illness, starvation, and dehydration.
Eyes and Vision
To maintain optimum vision, people need to have their eyes examined regularly throughout life. It is recommended that people under age 30 have their eyes tested every 3 to 5 years, or more frequently if there is a family history of diabetes, hypertension, blood dyscrasia, or eye disease (e.g., glaucoma). After age 40, an eye examination is recommended every 2 years. Assessment includes examination of the:
- External Structures
- Conjunctivitis is the inflammation of the bulbar and palpebral conjunctiva due to foreign bodies, chemicals, allergenic agents, bacteria, or viruses. Redness, itching, tearing, and mucopurulent discharge may occur that can produce crusting and matting of the eyelids during sleep.
- Dacryocystitis is the inflammation of the lacrimal sac manifested by tearing and a discharge from the nasolacrimal duct.
- Hordeolum (sty) is a redness, swelling, and tenderness of the hair follicle and glands that empty at the edge of the eyelids
- Iritis is the inflammation of the iris that may be caused by local or systemic infections and results in pain, tearing, and photophobia.
- “Black Eyes” may result from contusions or hematomas resulting from injury.
- Cataracts is an opacity of the lens or its capsule, common in those over the age of 65, or in newborns whose mothers contracted rubella in the first trimester of pregnancy (congenital cataracts).
- Glaucoma: a disturbance in the circulation of aqueous fluid, which causes an increase in intraocular pressure is the most frequent cause of blindness in people over age 40. It can be controlled if diagnosed early. Danger signs of glaucoma include blurred or foggy vision, loss of peripheral vision, difficulty of focusing on close objects, difficulty adjusting to dark rooms, and seeing rainbow-colored rings around lights.
- Ptosis: drooping of one eyelid at or below the pupil margin related to aging, edema from drug allergy or systemic disease, congenital lid muscle dysfunction, neuromuscular disease (e.g., myasthenia gravis), and third cranial nerve impairment.
- Ectropion: eversion; outturning of the eyelid
- Entropion: inversion; inturning of the eyelid
- Mydriasis: enlargement (dilation) of the pupils; occurs in injury, glaucoma, or drugs.
- Miosis: constriction of the pupils; occurs in iritis and opioid and narcotic agents.
- Anisocoria: marked inequality between pupil sizes
- Visual acuity is the degree of detail the eye can discern in an image.
- Snellen Standard Chart: standard tool used to test distance vision
- Preschool Children’s Chart: a pictographic variant of Snellen standard chart
- Snellen E Chart: Snellen variant used for illiterate individuals
- Rosenbaum Chart: a hand-held chart positioned 14 inches from the eyes as a test for close vision
- Jaeger Chart
- Ocular movement
- Visual fields, the area an individual can see when looking straight ahead
Many people wear eyeglasses or contact lenses to correct common refractive errors of the lens of the eye. These errors include:
- Myopia: nearsightedness
- Hyperopia: farsightedness
- Presbyopia: age-related loss of elasticity of the lens and resultant farsightedness.
- Astigmatism: an uneven curvature of the cornea that prevents horizontal and vertical rays from focusing on the retina.
Ears and Hearing
Assessment of the ear includes direct inspection and palpation of the external ear, inspection of the internal parts of the ear by an otoscope, and determination of auditory acuity. The process of “hearing” is a complex process. Sound can be detected by the ear through two mediums—air (air conduction) and bone (bone conduction).
- Audiometric evaluations (measurement of hearing at various decibels) are recommended for children and older adults.
- Conductive hearing loss: interruption of transmission of sound waves through the outer and middle ear structures, such as in a perforated tympanum, impacted cerumen, swelling of the auditory canal, etc.
- Sensorineural hearing loss: inability to detect sound due to damage to the inner ear, the auditory nerve, or the hearing center in the brain.
- Mixed hearing loss is a combination of both conduction and sensorineural loss.
Hearing loss is the most common chronic health condition in the United States, and about 40 million adults have hearing loss resulting from nonoccupational exposure to loud noises. According to the CDC, as little as two minutes at a rock concert can cause hearing damage. Many adults are unaware that they have hearing loss.
Lifespan Considerations
- Infants must be assessed for gross hearing (universal newborn hearing screening). This is done by ringing a bell from behind the infant or having the parent call the child’s name to check for a response. The newborn should quiet to the sound and may open their eyes wider. By 3 to 4 months of age, the child will turn head and eyes toward the sound.
- Children: at less than 3 years old, pull the pinna down and back to assess the external canal. Beyond 3 years of age, the pinna is pulled up and back.
- Adolescents: noise-induced hearing loss is becoming increasingly common in adolescents due to prolonged use of headsets at extremely high volumes plus environmental noise. Teach that music loud enough to prevent hearing a normal conversation can damage hearing.
- Older Adults: sensorineural hearing loss occurs. A quiet place must be used for examination. Generalized hearing loss occurs across all frequencies, but it often begins with high-frequency sounds (“f”, “s”, “sh”, “ph”). Conversation can become distorted and result in what appears to be inappropriate or confused behavior.
Nose and Sinuses
The nurse can inspect the nasal passages very simply with a flashlight or penlight. Assessment of the nose includes inspection and palpation of the external nose (the upper third of the nose is bone; the remainder is cartilage) and patency of the nasal cavities.
- Any reported problems with smell may warrant the nurse to test for the patient’s sense of smell.
| Assessment | Normal Findings | Deviations from Normal |
|---|---|---|
| Inspect the external nose for any deviations in shape, size, or color and flaring or discharge from the nares. | Symmetric, straight, no discharge, no flaring, uniform color | Asymmetric, discharge from nares, localized areas of redness or presence of skin lesions. |
| Lightly palpate the external nose to determine any areas of tenderness, masses, and displacements of bone and cartilage. | Not tender; no lesions | Tenderness on palpation; presence of lesions |
| Determine patency of both nasal cavities. Ask the client to close the mouth, exert pressure on one naris, and breathe through the opposite naris. Repeat the procedure to assess patency of the opposite naris. | Air moves freely as the client breathes through the nares | Air movement is restricted in one or both nares |
| Observe for the presence of redness, swelling, growths, and discharge. | Mucosa pink Clear, watery discharge No lesions | Mucosa red, edematous Abnormal discharge Presence of lesions |
| Inspect the nasal septum between the nasal chambers. | Nasal septum intact and in midline | Septum deviated |
| Palpate the maxillary and frontal sinuses for tenderness. | Not tenderness | Tenderness in one or more sinuses |
Lifespan Considerations
- Infants and Children:
- Push the tip of the nose gently upward with the thumb and shine a light into the nares.
- Ethmoid and maxillary sinuses are present at birth; frontal sinuses begin to develop by 1 to 2 years of age; and sphenoid sinuses develop later in childhood. Infants and young children have fewer sinus problems than older children and adolescents.
- Ethmoid sinuses continue to develop until age 12.
- Cough and runny nose are the most common signs of sinusitis in preadolescent children. Adolescents with sinusitis may have headaches, facial tenderness, and swelling.
- Older Adults: sense of smell becomes markedly diminished due to decreased number of and atrophy of olfactory nerve fibers.
- Nosebleeds may occur due to hypertensive disease or other arterial vessel changes.
Mouth and Oropharynx
The mouth and oropharynx are composed of a number of structures. Assessment is mainly done with inspection.
- Dental Caries
- Periodontal Disease (Pyorrhea) is characterized by gingivitis—red, swollen gingiva, bleeding, receding gum lines, and the formation of pockets between the teeth and gums.
- Plaque: invisible soft film that adheres to the enamel surface of teeth; it consists of bacterial, molecules of saliva, and remnants of epithelial cells and leukocytes.
- Tartar (dental calculus): if plaque is left unchecked, tartar forms. It is a visible, hard deposit of plaque and dead bacterial that forms at the gum lines.
- Glossitis: inflammation of the tongue.
- Stomatitis: inflammation of the oral mucosa.
- Parotitis: inflammation of the parotid salivary gland.
- Mouth Sores (canker sores, cold sores, fever blisters)
- Sordes: accumulation of foul matter (food, microorganisms, epithelial elements) on the teeth and gums
Lifespan Considerations
- Infants:
- Inspect the palate and uvula for a cleft. A bifid (forked) uvula may indicate an unsuspected cleft palate.
- Newborns may have pearly white nodules (epstein pearls) on their gums, which resolve without treatment.
- The first teeth erupt at about 6 to 7 months of age. Dental hygiene should be performed; assess adequate dental care by the parents. Cleansing of the infant’s teeth should be done daily with a soft cloth or soft toothbrush.
- Fluoride supplements should be given by 6 months if the child’s drinking water contains less than 0.3 parts per million (ppm) fluoride.
- Children should see a dentist by 1 year of age.
- Children:
- Tooth development should be appropriate for age.
- White spots on the teeth may indicate excessive fluoride ingestion.
- Drooling is common up to 2 years of age.
- The tonsils are normally larger in children than in adults and commonly extend beyond the palatine arch until the age of 11 or 12 years.
- Older Adults:
- Oral mucosa may be drier from decreased salivary gland activity or medications.
- Gum recession may occur, giving an appearance of increased toothiness.
- Taste sensations diminish due to taste bud atrophy and a decreased sense of smell, also related to decreased function of the fifth and seventh cranial nerves.
- Tiny purple or bluish black swollen areas under the tongue, known as caviar spots, are not uncommon. They are varicosities.
- Teeth may show signs of staining, erosion, chipping, and abrasions from loss of dentin. Older adults with limited income may delay or avoid professional dental care.
- Tooth loss occurs as a result of dental disease but is preventable with good dental hygiene.
- Check that full or removable dentures fit properly. Bone loss and weight loss or gain can change the way these prosthetics fit. Older adults may also fail to receive dental care (for both natural teeth and dentures) if they are homebound or in long-term care facilities.
- The gag response may be slightly sluggish.
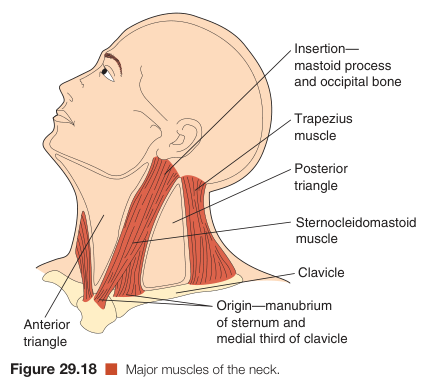
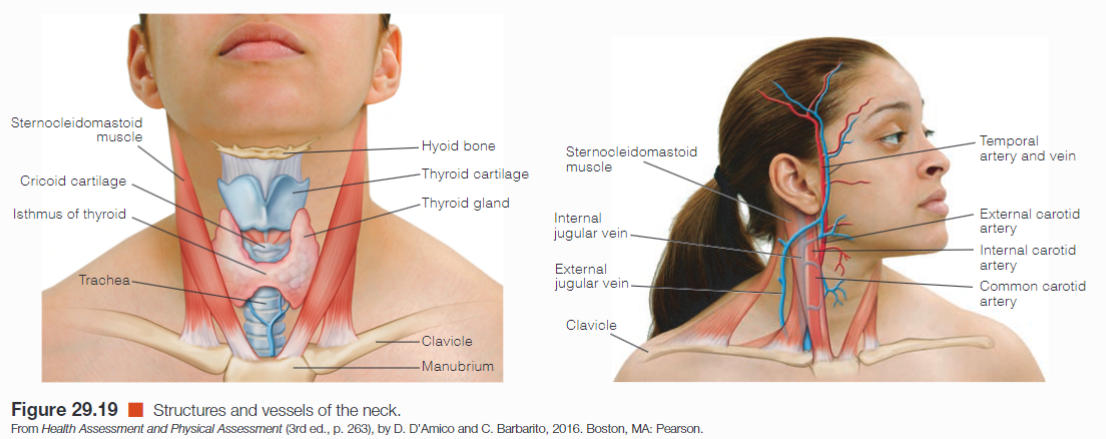
Neck
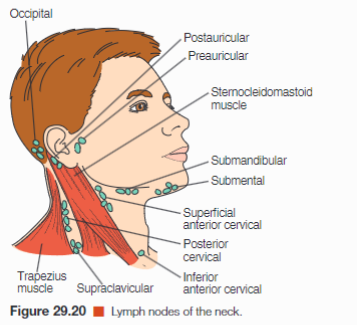
Examination of the neck includes the muscles, lymph nodes, trachea, thyroid gland, carotid arteries, and jugular veins. The areas of the neck are defined by the sternocleidomastoid muscles, which divide each side of the neck into two triangles: the anterior and posterior triangle.
- The trachea, thyroid gland, anterior cervical nodes, and carotid artery lie within the anterior triangle; the carotid artery runs parallel and anterior to the sternocleidomastoid muscle.
- The posterior lymph nodes lie within the posterior triangle.
- Each sternocleidomastoid muscle extends from the upper sternum (sterno-) and the medial third of the clavicle (-cleido-) to the mastoid process (-mastoid).