References:
- Kozier & Erb’s Fundamentals of Nursing: Concepts, Process, and Practice, 11th Edition, ISBN 9780135428733, by Audrey Berman, Shirlee J. Snyder, and Geralyn Frandsen (Ch. 35, pp. 854–856)
Oral
The oral route is preferred for opioids because of ease of administration. Because the duration of action of most opioids is approximately 4 hours, people with chronic pain have had to awaken during the night to medicate themselves for pain. To avoid this problem, long-acting or sustained-release formulations of morphine with a duration of 8 or more hours have been developed.
- An example of a long-acting morphine is MS Contin, a controlled release tablet. Clients receiving long-acting morphine may also need prn “rescue” doses of immediate-release analgesics such as Actiq, the short-acting oral transmucosal fentanyl citrate (OTFC) for acute breakthrough pain.
- Another method of oral opiate delivery is high-concentration liquid morphine. This formulation enables clients who can swallow only small amounts to continue taking the drug orally.
Transnasal
Transnasal administration has the advantage of rapid action of the medication because of direct absorption through the vascular nasal mucosa. A commonly used agent is butorphanol (Stadol) for acute migraines. Treating migraines via the nasal route is particularly beneficial because of the nausea, vomiting, and gastroparesis that can occur with migraines, making oral medications contraindicated.
Transdermal
Transdermal drug therapy is advantageous in that it delivers a relatively stable plasma drug level and is noninvasive. Fentanyl is a lipophilic synthetic opioid (i.e., binds to subcutaneous fat) and is available as a skin patch with various dosages (12 to 100 mcg). It provides drug delivery for up to 72 hours.
Fentanyl
The nurse must remember that fentanyl is 100 times more potent than morphine and is ordered in micrograms (mcg) not milligrams (mg).
The transdermal route is distinguished from the topical route in that the effects of the medications are systemic after the medication is absorbed.
- Nurses must teach clients not to use heat (e.g., hot tubs, heating pads) with the fentanyl patch, because increased absorption may result. A client with a fever may absorb the medication faster because of the vasodilation from the increased skin temperature.
- Used patches should be disposed of in a tamper-proof container. This is especially true in the home setting because a used patch can contain enough residual medication to harm a small child or animal if ingested.
Transmucosal
Many clients with cancer-related pain experience breakthrough pain even though they are on a fixed schedule for pain control. The transmucosal route is helpful for breakthrough pain because the oral mucosa is well vascularized, which helps with rapid absorption. Two forms of fentanyl are available for transmucosal delivery: oral transmucosal fentanyl citrate (OTFC; Actiq) and a fentanyl buccal tablet (Fentora).
Rectal
Some opioid medicines are available in suppository form. The rectal route is particularly useful for clients who have dysphagia (difficulty swallowing) or nausea and vomiting. An example is the belladonna and opium suppositories, which are used to relieve moderate to severe pain caused by ureteral spasm.
Subcutaneous
Although the subcutaneous route has been used extensively to deliver opioids, another technique uses subcutaneous catheters and infusion pumps to provide continuous subcutaneous infusion (CSCI) of opioids. CSCI is particularly helpful for clients (a) whose pain is poorly controlled by oral medications, (b) who are experiencing dysphagia or GI obstruction, or (c) who have a need for prolonged use of parenteral opioids. CSCI involves the use of a small, light, battery-operated pump that administers the drug through a 23- or 25-gauge butterfly needle. The needle can be inserted into the anterior chest, the subclavicular region, the abdominal wall, the outer aspects of the upper arms, or the thighs. Client mobility is maintained with the application of a shoulder bag or holster to hold the pump. The site is rotated every 7 days and medication infusion rates are usually 3 to 5 mL per hour.
Intramuscular
The intramuscular (IM) route should not be used for administration of analgesics.
Disadvantages
Disadvantages include variable absorption and unpredictable onset of action and peak effect, as well as the tissue damage that may result, even if properly administered. Regardless of precautions taken, there is pain involved with administration.
Intravenous
The IV route provides the most rapid onset for pain relief with few side effects. However, just as the onset of pain relief occurs in 5 to 10 minutes, so can adverse effects, such as respiratory depression. The analgesic can be administered by IV bolus or by continuous infusion. IV medications should be given slowly to decrease adverse effects. Caution is needed to prevent the introduction of air or bacteria into the tubing, and to prevent the introduction of medications that are incompatible with other medications dissolved in the IV solution.
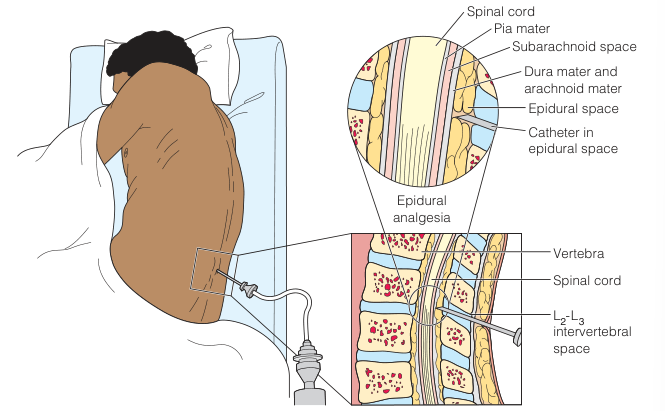
Intraspinal
Another method of delivery is the infusion of opioids into the epidural or intrathecal (subarachnoid) space. Intraspinal infusion may be administered to clients who require pain management in a variety of practice settings (e.g., acute care, outpatient, and home care).
- Analgesics administered via the intraspinal route are delivered adjacent to the opioid receptors in the dorsal horn of the spinal cord. Two commonly used medications are morphine sulfate and fentanyl.
- All medicines administered via the intraspinal route need to be sterile and preservative free (preservatives are neurotoxic).
Advantages
The major benefit of intraspinal drug therapy is:
- Superior analgesia with less medication used.
- The epidural space is most commonly used because the dura mater acts as a protective barrier against infection, including meningitis, and there is less risk of developing a “spinal headache.”
- Intraspinal catheters are not in constant contact with blood; thus, an infusion can be stopped and restarted later without concern that the catheter is no longer patent.
Intrathecal Route
Intrathecal administration delivers medication directly into the cerebrospinal fluid (CSF, located in the subarachnoid space) that bathes and nourishes the spinal cord.
- Medicines quickly bind to the opioid receptor sites in the dorsal horn when administered in this fashion, speeding the onset and peak effect, while prolonging the duration of action of the analgesic.
- Very little drug is absorbed by blood vessels into the systemic circulation. In fact, the drug must circulate through the CSF to be excreted. As a result, there may be a delayed onset (24 hours following the administration) of respiratory depression, because medication that has left the spinal opioid sites travels through the brain to be eliminated.
Route-Potency Relationships
An example of how the route of administration affects the relative potency of opioids is as follows: A client who requires 300 mg of oral morphine per day to control pain will need 100 mg of parenteral morphine, 10 mg of epidural morphine, and only 1 mg of intrathecal morphine in a 24-hour period.
Epidural Route
In contrast, the epidural infusion requires a higher dose of opioid to create the desired effect, which can produce adverse effects of itching, urinary retention, and respiratory depression. Often, an opioid (e.g., fentanyl) and a local anesthetic (e.g., bupivacaine) are combined to lower the dose of opioid needed. As a result, there may be an increase in fall risk for some clients who develop muscular weakness in their legs or orthostatic hypotension in response to the local anesthetic.
Opioid Antagonist
As a precaution, have naloxone (Narcan), sodium chloride 0.9% diluent, and injection equipment on hand for each client receiving an opioid-containing epidural infusion.
Catheter Insertion
The anesthesiologist or nurse anesthetist inserts a needle into the intrathecal or epidural space (typically in the lumbar region) and threads a catheter through the needle to the desired level. The catheter is connected to tubing that is then positioned along the spine and over the client’s shoulder for the nurse to access. The entire catheter and tubing are taped securely to prevent dislodgment. Often an occlusive, transparent dressing is placed over the insertion site for easy identification of catheter displacement or local inflammation.
- Temporary catheters, used for short-term acute pain management, are usually placed at the lumbar or thoracic vertebral level and usually removed after 2 to 4 days.
- Permanent catheters, for clients with chronic pain, may be tunneled subcutaneously through the skin and exit at the client’s side or be connected to a pump implanted in the abdomen. Tunneling of the catheter reduces the risk of infection and displacement of the catheter.
After the catheter is inserted, the nurse is responsible for monitoring the infusion and assessing the client per institutional policy.
Continuous Local Anesthetics
Continuous subcutaneous administration of long-acting local anesthetics into or near a surgical site is a technique that can be used to provide postoperative pain control. This technique has been used for a variety of surgical procedures, including knee arthroplasty, abdominal hysterectomy, hernia repair, and mastectomy. Nursing interventions for the client with infusion of a continuous local anesthetic include the following:
- Conduct pain assessment and documentation every 2 to 4 hours while the client is awake.
- Check the dressing every shift to ensure it is intact. The dressing is not usually changed in order to avoid dislodging the catheter. Contact the primary care provider if the dressing becomes loose.
- Check the site of the catheter. It should be clean and dry.
- Assess the client for signs of local anesthetic toxicity (e.g., cardiac arrhythmias, dizziness; ringing in the ears; a metallic taste; tingling or numbness of the lips, gums, or tongue) or neurologic deficit distal to the catheter insertion site.
- Notify the primary care provider of signs of local anesthetic toxicity or neurologic deficit. If detected early, prompt treatment should be initiated in order to prevent serious complications.