References:
- Kozier & Erb’s Fundamentals of Nursing: Concepts, Process, and Practice, 11th Edition, ISBN 9780135428733, by Audrey Berman, Shirlee J. Snyder, and Geralyn Frandsen (Ch. 36, pp. 915–956)
On Hold
I’m planning on adapting this entire chapter, but I’ve limited it to Types of Wounds, Pressure Injuries, and Wound Healing at the moment.
The skin is the largest organ in the body and serves a variety of important functions in maintaining health and protecting the individual from injury. Important nursing functions are maintaining skin integrity and promoting wound healing. Impaired skin integrity is not a frequent problem for most healthy individuals but is a threat to older adults; to clients with restricted mobility, chronic illnesses, or trauma; and to those undergoing invasive healthcare procedures.
Types of Wounds
- Intentional trauma occur during therapy, such as operations. Although removing a tumor, for example, is therapeutic, the surgeon must cut into body tissues, thus traumatizing them.
- Unintentional wounds are accidentally; for example, a client may fracture an arm in an automobile collision.
- Closed wounds are wounds that do not breach the skin, such as a fracture that does not break the skin.
- Open wounds are wounds that break the skin or mucous membrane surface.
Wounds can also be describe based on how they were acquired:
- Incision: an open wound, deep or shallow, that is caused by a sharp instrument.
- Contusion: a closed wound where the skin appears ecchymotic (bruised) because of damaged blood vessels. This is caused by a blow from a blunt instrument.
- Abrasion: an open wound involving the skin caused by scraping.
- Puncture: an open wound caused by penetration of the skin and underlying tissues by a sharp instrument.
- Laceration: an open wound with jagged edges due to tissues being torn apart, often from accidents.
- Penetrating wounds: an open wound caused by penetration of the skin and underlying issues, often unintentionally. This differs from puncture wounds as it can be caused by objects that aren’t “sharp”, such as metal fragments or a bullet.
Wounds may be described according to the likelihood and degree of wound contamination and depth:
- Clean wounds are uninfected wounds in which there are minimal inflammation and the gastrointestinal, genital, and urinary tracts are not entered. Clean wounds are primarily closed wounds.
- Clean-contaminated wounds are surgical wounds in which the gastrointestinal, genital, or urinary tract has been entered. Such wounds show no evidence of infection.
- Contaminated wounds include open, accidental, and surgical wounds involving a major break in sterile technique or spillage from the gastrointestinal tract. Contaminated wounds show evidence of inflammation.
- Dirty or infected wounds include wounds with evidence of a clinical infection, such as purulent drainage or necrosis.
- Partial thickness wounds are confined to the skin, that is, the dermis and epidermis, and heal by regeneration.
- Full thickness wounds involve the dermis, epidermis, subcutaneous tissue, and possibly muscle and bone, and require connective tissue repair.
Pressure Injuries
Pressure injuries consist of injury to the skin or underlying tissue, usually over a bony prominence, as a result of force alone or in combination with movement. They were previously called pressure ulcers, decubitus ulcers, pressure sores, or bed sores. This problem presents in both acute and long-term care settings.
Because healthcare-associated pressure injuries are substantially preventable, public health insurance—and increasing numbers of private health insurance companies—will no longer reimburse healthcare agencies for the cost of treating them. In addition, development of a stage 3 or 4 or unstageable pressure injury (see later in this page) is considered a serious reportable event.
2019 The Joint Commission National Patient Safety Goal #14
Goal 14: Prevent Healthcare–Associated Pressure Ulcers
- Assess and periodically reassess each patient’s and resident’s risk for developing a pressure ulcer and take action to address any identified risks. Rationale: Pressure ulcers (decubiti) continue to be problematic in all health care settings. Most pressure ulcers can be prevented, and deterioration at stage 1 can be halted. The use of clinical practice guidelines can effectively identify residents and define early intervention for prevention of pressure ulcers.
Etiology of Pressure Injuries
- Pressure injuries are due to localized ischemia, a deficiency in the blood supply to the tissue. The tissue is compressed between two surfaces, usually the surface of furniture such as the bed or chair and the bony skeleton.
- When blood cannot reach the tissue, the cells are deprived of oxygen and nutrients, the waste products of metabolism accumulate in the cells, and the tissue consequently dies. Prolonged, unrelieved pressure also damages the small blood vessels.
- After the skin has been compressed, it appears pale (blanched), as if the blood had been squeezed out of it. When pressure is relieved, the skin takes on a bright red flush (erythema), called reactive hyperemia.
- In dark-skinned clients, both the blanch and flush may be difficult to detect. Compare the reactions of questionable areas with other parts of the client’s skin. The flush is due to vasodilation, a process in which extra blood floods to the area to compensate for the preceding period of impeded blood flow.
- Reactive hyperemia usually lasts one-half to three-quarters as long as the duration of impeded blood flow to the area. If the redness disappears in that time, no tissue damage is anticipated. If, however, the redness does not disappear, then tissue damage has occurred.
Risk Factors
Several factors contribute to the formation of pressure injuries: friction and shearing, immobility, inadequate nutrition, fecal and urinary incontinence, decreased mental status, diminished sensation, excessive body heat, advanced age, and the presence of certain chronic conditions.
- Friction and Shearing: Friction is a force acting parallel to the skin surface. For example, sheets rubbing against skin create friction. Friction can abrade the skin, that is, remove the superficial layers, making it more prone to breakdown.
- Shearing force is a combination of friction and pressure. It occurs commonly when a client assumes a sitting position in bed. In this position, the body tends to slide downward toward the foot of the bed. This downward movement is transmitted to the sacral bone and the deep tissues. At the same time, the skin over the sacrum tends not to move because of the adherence between the skin and the bed linens. The skin and superficial tissues are thus relatively unmoving in relation to the bed surface, whereas the deeper tissues are firmly attached to the skeleton and move downward. This causes a shearing force in the area where the deeper tissues and the superficial tissues meet. The force damages the blood vessels and tissues in this area.
- Immobility: Immobility refers to a reduction in the amount and control of movement an individual has. Normally individuals move when they experience discomfort due to pressure on an area of the body. However, paralysis, extreme weakness, pain, or any cause of decreased activity can hinder an individual’s ability to change positions independently and relieve the pressure, even if the individual can perceive the pressure.
- Inadequate Nutrition: Weight loss, muscle atrophy, and loss of subcutaneous tissue reduce the amount of padding between the skin and the bones, increasing the risk of pressure injury development. More specifically, inadequate intake of protein, carbohydrates, fluids, zinc, and vitamin C contributes to pressure injury formation.
- Hypoproteinemia predisposes the client to dependent edema. This makes the skin more prone to injury by decreasing its elasticity, resilience, and vitality. Edema increases the difference between the capillaries and the cells, thereby slowing the diffusion of oxygen to the tissue cells and of metabolites away from the cells.
- Fecal and Urinary Incontinence: Moisture from incontinence promotes skin maceration (tissue softened by prolonged wetting or soaking) and makes the epidermis more easily eroded and susceptible to injury. Digestive enzymes in feces, urea in urine, and gastric tube drainage also contribute to skin excoriation (area of loss of the superficial layers of the skin; also known as denuded area).
- Any accumulation of secretions or excretions (including sweat) is irritating to the skin, harbors microorganisms, and makes an individual prone to skin breakdown and infection. Skin or tissue injury due primarily to moisture is referred to as moisture-related skin damage (MASD) or incontinence-associated dermatitis (IAD). MASD or IAD can be considered “outside-in” damage where true pressure injuries would be considered “inside-out.”
- Decreased Mental Status: Individuals with a reduced level of awareness, for example, those who are unconscious, are heavily sedated, or have dementia, are at risk for pressure injuries because they are less able to recognize and respond to pain associated with prolonged pressure.
- Diminished Sensation: Paralysis, stroke, or other neurologic disease may cause loss of sensation in a body area. Loss of sensation reduces an individual’s ability to respond to trauma, to injurious heat and cold, and to the tingling (“pins and needles”) that signals loss of circulation.
- Excessive Body Heat: Elevated body temperature increases metabolic rate, increasing tissue oxygen needs. Infection accompanying the elevated body temperature can also affect the body’s ability to deal with the effects of tissue compression.
- Advanced Age: The aging process brings about several changes in the skin and its supporting structures, making the older adult more prone to impaired skin integrity. These changes include the following: loss of lean body mass, generalized thinning of the epidermis, decreased strength and elasticity from changes in collagen, increased dryness due to decreased oil production in sebaceous glands, diminished pain perception, and diminished venous and arterial flow.
- Chronic Medical Conditions: Certain chronic conditions such as diabetes and cardiovascular disease are risk factors for skin breakdown and delayed healing. These conditions compromise oxygen delivery to tissues by poor perfusion and thus cause poor and delayed healing and increase risk of pressure injuries.
- Other Factors: Other factors contributing to the formation of pressure injuries are poor lifting and transferring techniques, incorrect positioning, hard support services, and incorrect application of pressure-relieving devices.
Stages of Pressure Injuries
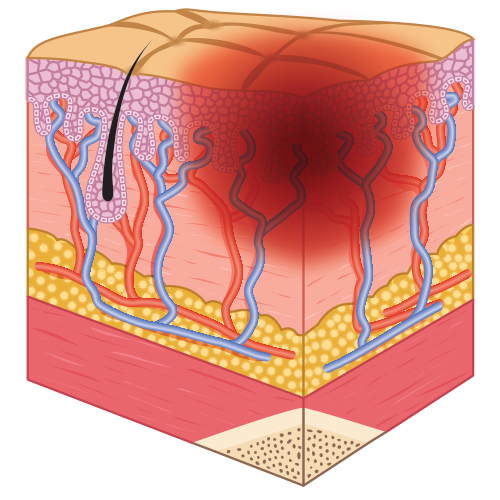
- Stage 1: skin is unbroken and reddened, but does not blanch.
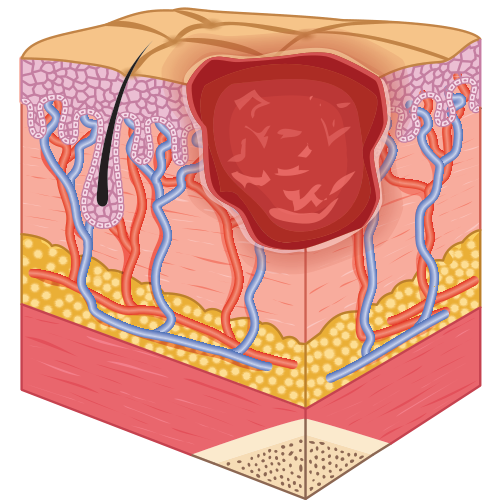
- Stage 2: partial-thickness skin loss.
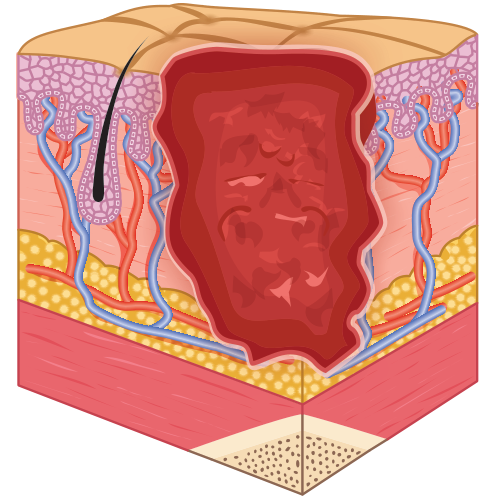
- Stage 3: full-thickness skin loss and damage that may reach as deeply as the fascia.
- Stage 3 with epibole (the edges of the skin surrounding the injury roll under and the damage extends under the rolled tissue).
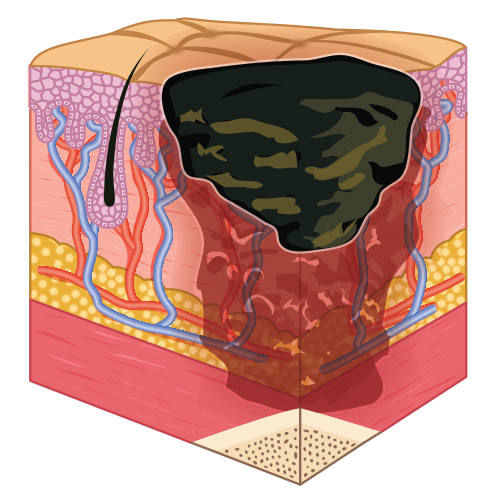
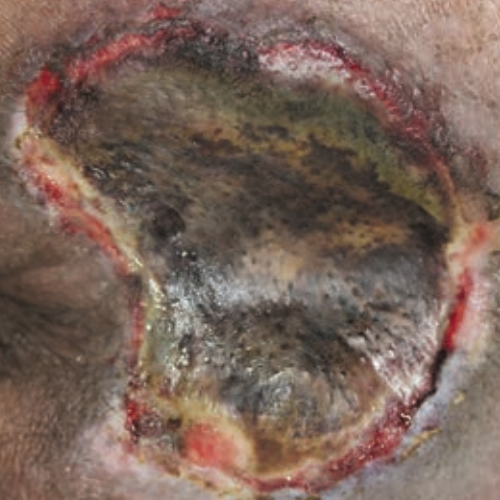
- Stage 4: full-thickness skin loss with tissue death or damage to underlying structures.
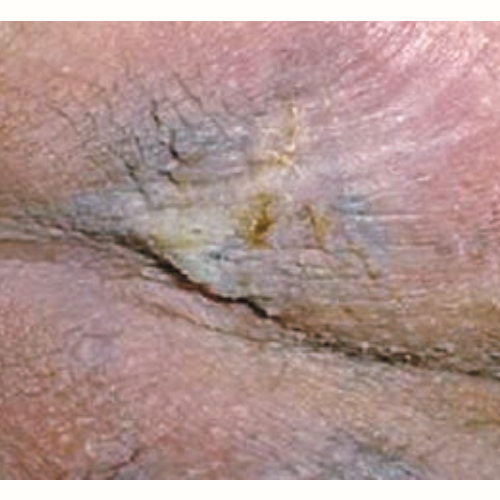
- Unstageable or unclassified: full-thickness loss. The full extent of the injury cannot be determined due to slough or eschar.
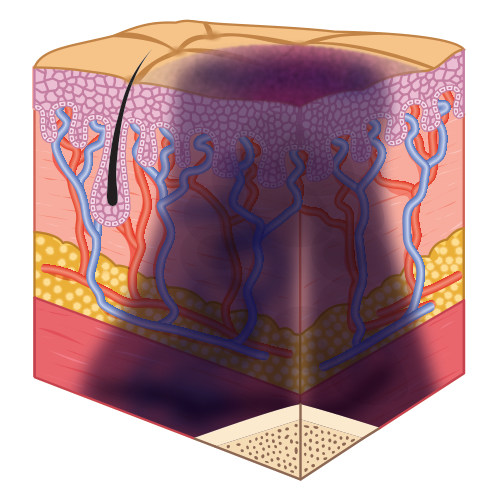
- Deep tissue pressure injury–depth unknown: dark area of discolored intact skin due to damage of underlying soft tissue.



Risk Assessment Tools
Pressure injuries are the most common and most preventable among the different alterations in skin integrity. The Braden and Norton tools should be used when the client first enters the healthcare agency and whenever the client’s condition changes. In some long-term care facilities, a risk assessment using the Braden or Norton scale is conducted on admission and then on a regular basis, usually weekly. This increases awareness of specific risk factors and serves as assessment data from which to plan goals and interventions to either maintain or improve skin integrity.
Braden Scale
The Braden Scale for Predicting Pressure Sore Risk consists of six subscales: sensory perception, moisture, activity, mobility, nutrition, and friction and shear. A total of 23 points is possible:
- An adult who scores below 18 or 19 points is generally considered at risk. For best results, nurses should be trained in proper use of the scale.
- Scores of 15 or 16 should be viewed as indicators, not predictors, of risk—i.e., the patient is already at risk.
Norton’s Pressure Area Risk Assessment Form
| Factor | Score 1 | Score 2 | Score 3 | Score 4 |
|---|---|---|---|---|
| A. General Physical Condition | Good | Fair | Poor | Very bad |
| B. Mental State | Alert | Apathetic | Confused | Stuporous |
| C. Activity | Ambulatory | Walks with help | Chairbound | Bedfast |
| D. Mobility | Full | Slightly limited | Very limited | Immobile |
| E. Incontinence | Absent | Occasionally | Usually urinary | Double |
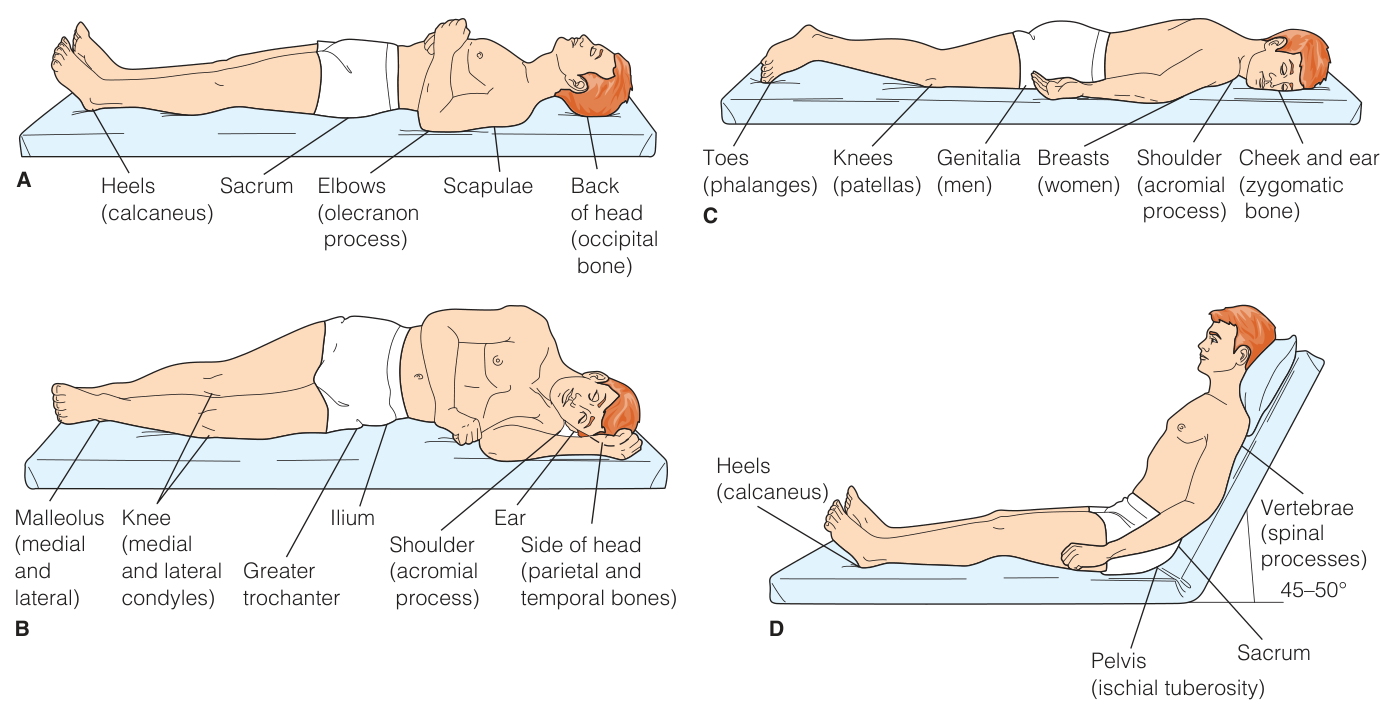
Assessing Common Pressure Sites
- Ensure the lighting is good, preferably natural or fluorescent, because incandescent lights can create a transilluminating effect.
- Regulate the environment before beginning the assessment so that the room is neither too hot nor too cold. Heat can cause the skin to flush; cold can cause the skin to blanch or become cyanotic.
- Inspect pressure areas (see below) for discoloration. This can be caused by impaired blood circulation to the area. The pressure areas should have brisk capillary refill when gently pressed with a finger or thumb.
- Inspect pressure areas for abrasions and excoriations. Abrasions can occur when skin rubs against a sheet. Excoriations can occur when the skin has prolonged contact with body secretions or excretions or with dampness in skinfolds.
- Palpate the surface temperature of the skin over the pressure areas (warm your hands first). Normally, the temperature is the same as that of the surrounding skin. Increased temperature is abnormal and may be due to inflammation.
- Palpate over bony prominences and dependent body areas for the presence of edema, which feels spongy or boggy.
Wound Healing
Healing is a quality of living tissue; it is also referred to as regeneration (renewal) of tissues. Healing can be considered in terms of types of healing, having to do with the primary care provider’s decision on whether to allow the wound to seal itself or to purposefully close the wound, and phases of healing, which refer to the steps in the body’s natural processes of tissue repair. The phases are the same for all wounds, but the rate and extent of healing depends on factors such as the type of healing, the location and size of the wound, and the health of the client.
Types of Wound Healing
The types of healing are influenced by the amount of tissue loss.
- Primary intention healing occurs where the tissue surfaces have been approximated (closed) and there is minimal or no tissue loss; it is characterized by the formation of minimal granulation tissue and scarring.
- Also called primary union or first intention healing.
- Examples: closed surgical incision, use of tissue adhesive to seal clean lacerations or incisions
- Secondary intention healing involves a wound that is extensive and involves considerable tissue loss, and in which the edges cannot and should not be approximated.
- Secondary intention healing differs from primary intention by its (a) repair time being longer, (b) scarring is greater, and (c) susceptibility to infection is greater.
- Examples: pressure injury
- Wounds that are left open for 3 to 5 days to allow edema or infection to resolve or exudate to drain and are then closed with sutures, staples, or adhesive skin closures achieve tertiary intention healing. This is also called delayed primary intention.
Phases of Wound Healing
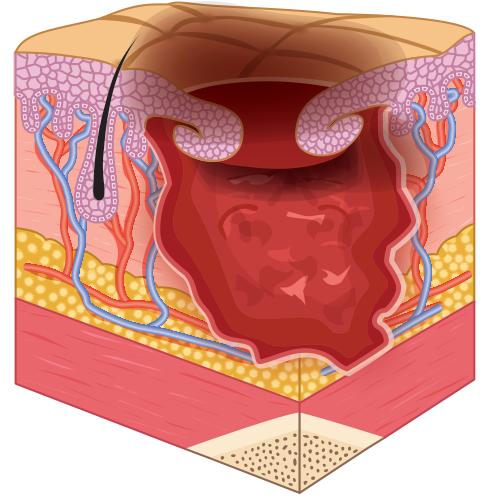
- The Inflammatory Phase begins immediately after injury and lasts 3 to 6 days. Two major processes, hemostasis and phagocytosis, occur during this phase:
- Hemostasis (the cessation of bleeding) results from vasoconstriction of the larger blood vessels in the affected area, retraction (drawing back) of injured blood vessels, the deposition of fibrin (connective tissue), and the formation of blood clots in the area. The blood clots provide a matrix of fibrin that becomes the framework for cell repair. A scab may also form on the surface of the wound, aiding hemostasis and inhibit wound contamination.
- During the inflammatory phase, the blood supply to the wound increases, bringing with it oxygen and nutrients needed in the healing process. The area appears reddened and edematous as a result. Exudate of fluid and cell debris is a normal accumulation and helps cleanse the wound. In surgical wounds, this lasts 1 to 3 days. Overproduction of this exudate and other factors can impair wound healing, especially in chronic wounds.
- During cell migration, leukocytes (specifically, neutrophils) move into the interstitial space. These are replaced after 24 hours after injury by macrophages. These macrophages engulf microorganisms and cellular debris by a process known as phagocytosis. The macrophages also secrete an angiogenesis factor, which stimulates the formation of epithelial buds at the end of injured blood vessels. The microcirculatory network that results sustains the healing process and the wound during its life. This inflammatory response is essential to healing. Measures that impair inflammation, such as steroid medications, can place the healing process at risk.
Types of Wound Exudate
Exudate is material, such as fluid and cells, which has escaped from blood vessels during the inflammatory process and is deposited in tissue or on tissue surfaces. The nature and amount of exudate vary according to the tissue involved, the intensity and duration of the inflammation, and the presence of microorganisms.
- Serous exudate consists chiefly of serum (the clear portion of blood). It looks watery and has few cells. An example is the fluid in a blister from a burn.
- Purulent exudate is thicker than serous exudate because of the presence of pus, which consists of leukocytes, liquefied dead tissue debris, and dead and living bacteria. The process of pus formation is referred to as suppuration. Purulent exudates vary in color, some acquiring tinges of blue, green, or yellow, depending on the causative organism.
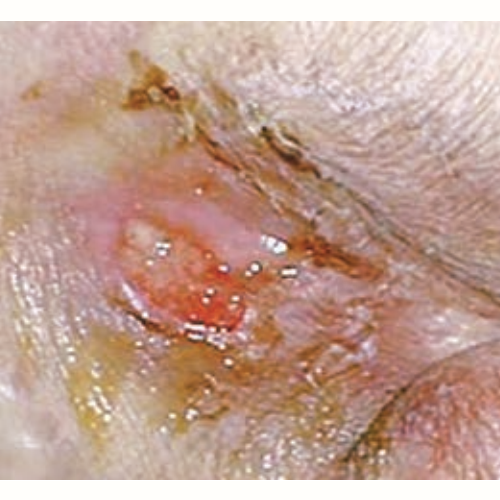
- Sanguineous exudate consists of large amounts of red blood cells, indicating damage to capillaries that is severe enough to allow the escape of red blood cells from plasma. This type of exudate is frequently seen in open wounds.
- Mixed types of exudate are often observed.
- A serosanguinous exudate consisting of both clear and blood-tinged drainage is commonly seen in surgical incisions.
- A purosanguinous discharge, consisting of pus and blood, is often seen in a new wound that is infected.
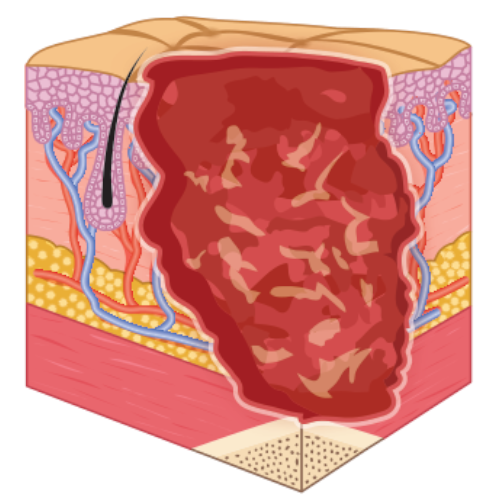
- The Proliferative Phase is the second phase of healing. It extends from day 3 to 4 to about 21 days postinjury. Fibroblasts (connective tissue cells), which migrate into the wound starting about 24 hours after injury, begin to synthesize collagen. Collagen is a whitish protein substance that adds tensile strength to the wound. As the amount of collagen increases, so does the strength of the wound; thus the change that the wound will remain closed progressively increases. If the wound is sutured, a raised “healing ridge” appears under the intact suture line. In a wound that is not sutured, the new collagen is often visible.
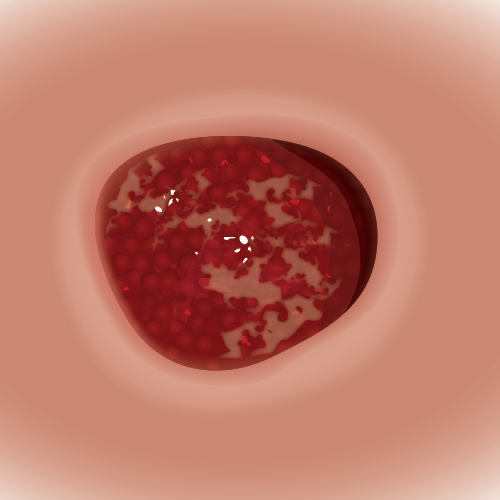
- Capillaries grow across the wound, increasing the blood supply. Fibroblasts move from the bloodstream to the wound, depositing fibrin. As the capillary network develops, the tissue becomes a translucent red color. This tissue, called granulation tissue, is fragile and bleeds easily.
- When the skin edges of a wound are not sutured, the area must be filled in with granulation tissue. When the granulation tissue matures, marginal epithelial cells migrate to it, proliferating over this connective tissue base to fill the wound.
- If the wound does not close by epithelialization, the area becomes covered with dried plasma proteins and dead cells. This is called eschar.
- Initially, wounds healing by secondary intention seep blood-tinged (serosanguineous) drainage. Later, if they are not covered by epithelial cells, they become covered with thick, gray, fibrinous tissue that is eventually converted into dense scar tissue.
- The Maturation or Remodeling Phase begins on about day 21 and can extend 1 or 2 years after the injury. Fibroblasts continue to synthesize collagen. The wound is remodeled and contracted. The scar becomes stronger but the repaired area is never as strong as the original tissue. In some individuals, particularly dark-skinned individuals, an abnormal amount of collagen is laid down. This can result in a hypertrophic scar, or keloid.