References:
- Maternal & Child Health Nursing: Care of the childbearing & childrearing family, 8th Edition, ISBN 978-149-63-4813-5, by JoAnne Silbert-Flagg and Adele Pillitteri (Ch. 21)
- Dr. RPS Maternal and Newborn Care: A Comprehensive Guide and Source Book for Teaching and Learning, 2nd Edition, ISBN 978-971-98-2265-3, by Rosalinda Parado Salustiano (Ch. 5, pp. 93–96)
- Comprehensive Nursing Licensure Review Book: Local and International Test Prep, Volume 1, ISBN 978-971-51-3383-8, by Josie Quiambao-Udan (Vol. 1, pp. 179–181)
- The Topranker’s Guide: A Comprehensive Study Guide for the Nurse Licensure Exam (p. 249)
- Lecturers
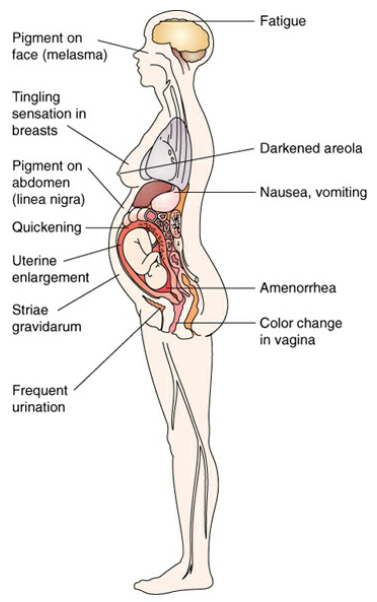
The signs of pregnancy are divided into three categories. Presumptive signs are those felt by the mother herself, probable signs are those observed by a healthcare provider, and positive signs are those emanating from the fetus itself. Succinctly, presumptive signs are subjective, probable signs are objective, and positive signs are documented.
Laboratory Tests
The commonly used laboratory tests for pregnancy are based on the use of a venipuncture of a urine specimen to detect the presence of human chorionic gonadotropin (hCG), a hormone created by the chorionic villi of the placenta, in the urine or blood serum of the pregnant woman. Because these tests are only accurate 95% to 98% of the time, positive results from these tests are considered probably rather than positive signs.
- Serum hCG can be measured by 7 to 9 days after conception (about 50 mIU/mL), but appear as early as 24 to 48 hours after implantation in trace amounts. They peak at about 100 mIU/mL on the 60th and 80th day of gestation, before declining until it is barely detectable in serum or urine by term.
- Home pregnancy tests: a number of brands are available over-the-counter tests that take only 2 to 3 minutes to complete. They have a high degree of accuracy (97%–99%) if the instructions are followed exactly because they can detect as little as 35 mIU/mL of hCG. For the test, a woman dips a reagent strip into her stream of urine. A color change or the appearance of two bars on the strip denotes pregnancy.
- Instructions usually include: check the expiration date; read the instruction pamphlet; the best time to test is in the morning (concentrated urine); read the test results at the exact time the instructions dictate; some medications can cause false positives; early prenatal care is the best safeguard to ensure a successful pregnancy.
Indications of Pregnancy
| Age of Gestation | Presumptive | Probable | Positive | Description |
|---|---|---|---|---|
| 1 | Maternal Serum Test | A venipuncture of blood serum reveals the presence of hCG | ||
| 2 | Breast Changes | Feeling of tenderness, fullness, tingling; enlargement and darkening of areola | ||
| 2 | Nausea, Vomiting | Nausea or vomiting on arising or when fatigued | ||
| 2 | Amenorrhea | Absence of menstruation | ||
| 3 | Frequent Urination | Sense of having to void more often than usual | ||
| 6 | Chadwick’s Sign | Color change of the vagina from pink to violet | ||
| 6 | Goodell’s Sign | Softening of the cervix | ||
| 6 | Hegar’s Sign | Softening of the lower uterine segment | ||
| 6 | Sonographic evidence of gestational sac | Characteristic ring is evident | ||
| 8 | Sonographic evidence of fetal outline | Fetal outline can be seen and measured by sonogram | ||
| 10–12 | Fetal heart audible | Doppler ultrasound reveals heartbeat | ||
| 12 | Fatigue | General feeling of tiredness | ||
| 12 | Uterine enlargement | Uterus can be palpated over symphysis pubis | ||
| 16 | Ballottement | When lower uterine segment is tapped on a bimanual examination, the fetus can be felt to rise against the abdominal wall | ||
| 18 | Quickening | Fetal movement felt by woman | ||
| 20 | Fetal movement felt by examiner | Fetal movement can be palpated through abdomen | ||
| 20 | Braxton Hicks contractions | Periodic uterine tightening occurs | ||
| 20 | Fetal outline felt by examiner | Fetal outline can be palpated through abdomen | ||
| 24 | Linea nigra | Line of dark pigment forms on the abdomen | ||
| 24 | Melasma | Dark pigment forms on face | ||
| 24 | Striae gravidarum | Stretch marks form on abdomen |
Presumptive signs are subjective; may be noticed by the women but are not conclusive proof of pregnancy, which are:
- Amenorrhea: first sign at two weeks from fertilization because of persistence of corpus luteum.
- Nausea and Vomiting: the most common forms of discomfort.
- Urinary Frequency: most disturbing sign, especially in the third trimester.
- Fatigue: from estrogen, in early pregnancy.
- Breast Changes: tingling of the nipples (4 weeks), darkening and enlargement of areola, enlargement of the breasts, and increased number of milk-secreting cells.
- Skin changes: chloasma, linea nigra, striae gravidarum, diaphoresis.
- Quickening, often felt stronger at 10 weeks.
- Leukorrhea: whitish, mucoid vaginal discharge due to estrogen.
- Weight increase: an unusual increase in weight not caused by a change in diet.
- Enlargement of the uterus.
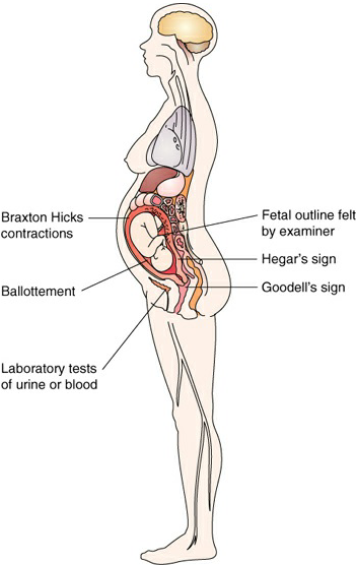
Probable signs are objective as noticed or observed by the healthcare provider but still not conclusive of pregnancy, which are:
- Abdominal enlargement from uterine growth.
- Fetal Parts via palpation by an examiner may actually be a tumor with calcium deposits. This does not constitute a sure sign of pregnancy.
- Goodell’s sign: softening of the cervix.
- Hegar’s sign: softening of the isthmus (lower uterine segment) and compressibility of the uterus.
- Chadwick’s sign: blue/purple discoloration of the cervix, vaginal mucosa, and perineum. This is caused by increased vascularization as a result of increased estrogen levels.
- Ladin’s Sign: softening of the uterus in the anterior midline along the utero-cervical junction.
- McDonald’s sign: the uterus becomes flexible at the uterocervical junction at 7-8 weeks
- Ballottement: rebound of the fetus against examiner’s fingers. This may also be simulated by a loosely attached uterine tumor and, therefore, is no more than a probable sign of pregnancy.
- Braxton Hicks contractions: irregular painless abdominal contractions relieved by walking (false labor). These may accompany any growing uterine mass; so, like ballottement, they are no more than a probable sign of pregnancy.
- Piskacek’s sign: irregular softening in the cornual (interstitial fallopian tube) area; it may be confused with uterine myoma or abnormal uterine development.
- Von Fernwald Sign: irregular softening of the fundus over the site of implantation at 4-5 weeks.
- Positive pregnancy test: due to the presence and rising levels of hCG in maternal blood and urine. This may still be a false positive, e.g. in a hydatidiform mole that produces hCG.
- Radioimmunoassay (RIA): test for the beta subunit of hCG, potentially accurate enough for the diagnosis of a pregnancy.
Positive signs are objective, emanate from the fetus, and are therefore conclusive for pregnancy. These include three areas—demonstration of fetal heart, fetal movements, and visualization of the fetus by ultrasound.
- Fetal Heart Tones (FHT):
- An ordinary stethoscope can hear a fetal heart beat at around the 18th to 20th week of pregnancy.
- Doppler instrumentation can detect fetal heart sounds as early as the 10th to 12th week of gestation.
- Ultrasounds can reveal a beating heart as early as the sixth to seventh week of pregnancy.
- An echocardiography can demonstrate a heartbeat as early as five weeks.
- Fetal Outline visualized by an ultrasound is the most common method for confirmation of pregnancy. If a woman is pregnant, a characteristic ring, indicating the gestational sac, will be revealed on an oscilloscope screen as early as the fourth to sixth week of pregnancy. This also provides information about the site of implantation and whether a multiple pregnancy exists. By the eighth week, a fetal outline can be seen so clearly that the crown-to-rump length can be measured to establish the gestational age of the pregnancy.
- Fetal movement as felt by the examiner. While the mother can feel fetal movements as early as 16 to 20 weeks of pregnancy, an objective examiner can discern fetal movements at about the 20th to 24th week of pregnancy (unless the woman is extremely obese). This is considered more reliable because a woman could mistake the movement of gas through her intestines as fetal movement.