References:
- Dr. RPS Maternal and Newborn Care: A Comprehensive Guide and Source Book for Teaching and Learning, 2nd Edition, ISBN 978-971-98-2265-3, by Rosalinda Parado Salustiano (pp. 222-261)
- Lecturer (V)
The woman in labor is called the parturient. The real cause of labor is unknown, but there are various theories of labor:
- Uterine Myometrial Irritability/Uterine Stretch Theory: considered as the most acceptable theory; when the uterine muscles get stretched with fetal growth and increasing amniotic fluid, it results in irritability and contractions to empty the contents of the uterus.
- Low Progesterone Theory/Progesterone Deprivation Theory: labor is said to start when progesterone (a uterine muscle relaxant) decreases and uterine muscle stimulants increase in late pregnancy.
- Oxytocin Theory: the pressure of the fetal head on the cervix in late pregnancy stimulates the posterior pituitary gland to secrete oxytocin, which causes uterine contractions.
- Estrogenic, Fetal Hormone, and Prostaglandin Theories: all of these have a stimulating effect on the uterine musculature, causing uterine contractility.
- Theory of Aging Placenta: as the placenta matures, more pressure is exerted on the fundal portion, the usual placental site, and the most contractile portion of the uterus. It is believed that the resultant diminished blood supply to the area causes contraction.
Premonitory Signs of Labor
- Lightening: the descent/dipping, dropping of the presenting part to the true pelvis. Engagement is not the same as lightening. The head is said to be “engaged” when the largest diameter of the presenting part passes through the pelvic inlet or the pelvic brim. This occurs earlier in primigravidas, at one to two weeks before labor, and later in multigravidas, at one to two days before labor. There are various signs of lightening:
- Relief of dyspnea
- Relief of abdominal tightness
- Increased frequency of urination, varicosities, and pedal edema because of pressure on the bladder and pelvic girdle
- Shooting pains down the legs because of the pressure on the sciatic nerves
- Increased amount of vaginal discharge
- Braxton Hicks Contractions are another sign, beginning 3 to 4 weeks before labor. They are painless and false labor contractions, appearing intermittently, irregularly, and non-progressively. They do not progress cervical dilatation or effacement, produce abdominal (not lumbosacral) discomfort, and can be relieved by walking and edema. They last anywhere from 30 to 120 seconds, maybe feeling like a wide belt tightening around the front of the abdomen.
- Increased maternal energy/burst of energy because of the hormone epinephrine
- Slight decrease in maternal weight by 2 to 3 lbs, 1 to 2 days before labor. Before labor, there is a drop in the blood level of progesterone, a water-retaining hormone, causing the excretion of retained fluid.
- Show: blood-tinged mucus discharged from the cervix shortly before or during labor.
- Ripening of the Cervix: becomes soft as butter.
- Rupture of the Bag of Waters: an occasional sign. It is an indication for hospitalization.
- Progressive Fetal Descent
- Increased backache and sacroiliac pressure due to fetal pressure.
| Criteria | True Labor | False Labor |
|---|---|---|
| Contractions | Regular, progressive | Irregular, non-progressive |
| Discomfort | Lumbo-sacral radiating to the front; increasing intensity | Abdominal |
| Cervix | Dilated; the most important sign | No dilatation |
| Walking | Intensifies contractions | No effect on contraction |
| Enema | Intensifies contractions | No effect on contraction |
| Show | Present and increasing | Absent |
Physiological Changes in Labor
- Dilatation: progressive opening/widening of the cervical os. It is expressed in centimeters, described as “opening”, “widening”, “enlarging”, or “increasing in diameter”. It specifically refers to the cervical external os (a cervical dilatation of 3 cm means the cervical external os is 3 cm open). 10 cm is a fully dilated cervix, the end of the first stage of labor.
- Effacement: thinning and obliteration of the cervical canal. It is expressed in percentage, described as “thinning”, “shortening”, or “narrowing”. A 100% effaced cervix is a fully effaced cervix where the cervical canal has become paper thin or is already absent.
- Physiologic Retraction Ring: the separation of the active, shorter, thicker upper uterine segment an the passive, longer, and thinner lower segment. The Bandl’s Ring is a pathologic retraction ring, formed when the upper uterine segment is as active as the lower segment; seen as an abdominal indentation ring, signifying impending rupture of the uterus if not managed.
Components of Labor
A successful labor depends on four integrated concepts, often referred to as the four Ps:
- The passage (a woman’s pelvis) is of adequate size and contour.
- The passenger (the fetus) is of appropriate size and in an advantageous position and presentation.
- The powers of labor (uterine factors) are adequate.
- The psyche, or a woman’s psychological state which may either encourage or inhibit labor. This can be based on her past life experiences as well as her present psychological state.
Power
- Uterine Contractions: the primary power of labor. An involuntary, rhythmical, regular activity of uterine musculature. It occurs intermittently by allowing for a period of uterine relaxation between contractions; uterine and maternal rest and restoration of uteroplacental circulation; sustained fetal oxygenation. This propels the presenting part downward or forward, and aids in progressing dilatation and effacement.
- Contractions increase maternal BP due to increased peripheral arteriole pressure. Measurement of BP should be between contractions to gain accurate results.
- Myometrial contractions constrict blood vessels, decreasing uteroplacental circulation. As such, prolonged uterine contractions can cause fetal hypoxia.
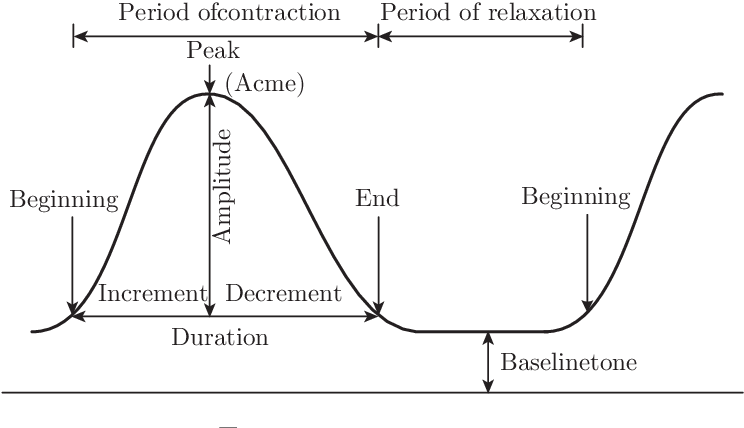
- Contractions can be graphed into three parts, and have relevant durations, intervals, and frequency:
- Increment: increasing or “building up” contraction; the first and longest phase.
- Acme: the apex, height, or peak of the uterine contractions.
- Decrement: the phase of decreasing contraction; “letting up”. The last/end phase.
- Duration: the period from increment to decrement. Measured in seconds.
- Contractions lasting more than 90 seconds can lead to fetal distress, and is called a tetanic contraction.
- Interval: the period from the end to the start of another contraction. It is the uterine resting time, and should be at least 1 minute, not less than 30 to 45 seconds. It is measured in minutes.
- Frequency: the period from the start of one contraction to the start of the next contraction. It is effectively duration plus the interval. Measured in minutes.
Palpation of Contractions
Place the hand lightly on the fundus with the fingers spread; described as mild, moderate and strong by judging the degree of indentability/depressability of the uterine wall during acme. If indentation is not possible, the contraction is strong; difficulty, moderate; and mild if tense but easily indented.
- An intrauterine catheter can be used to directly measure the strength of contractions. At acme, intensity ranges from 30 mm Hg to 55 mm Hg of pressure. The resting tonus average is 10 mm Hg. A major disadvantage of this method involves the requirement of a ruptured bag of water and invasiveness.
- Secondary Powers: maternal bearing down/pushing. Only done on full dilation (10 cm), and a fetal station of +1 (able to stimulate the Ferguson reflex, which is triggered by pressure on the pelvic floor).
- Bearing down should not be done prior to full dilation due to the risk of lacerations.
- Teach the mother to take a deep breath as soon as the next contraction begins, and then, with breath held, exert a downward pressure exactly as though she were straining at the stool. She should not hold her breath for longer than six seconds, during pushing. Involuntary pushing, grunting, groaning, exhaling, or breath-holding for less than seconds is supported. She should push four or more pushes per contraction.
Passenger
The passenger is the fetus. The body part of the fetus that has the widest diameter is the head, so this is the part least likely to be able to pass through the pelvic ring. Whether a fetal skull can pass depends on both its structure (bones, fontanelles, and suture lines) and its alignment with the pelvis.
- The fetal skull is composed of eight bones: the superior bones—frontal, two parietal, and occipital—and the inferior bones (sphenoid, ethmoid, temporal). The inferior bones are never the presenting part, so are not as important.
inc p. 747
Passage
The passage refers to the route a fetus must travel from the uterus through the cervix and vagina to the external perineum.
Divided between the soft passages—cervix, vagina, and perineum (potentially lacerated)—and bony passages—the pelvis. Problems of the bony pelvis that can influence the progress of labor include heredity, a contracted pelvis due to avitaminosis D or rickets in childhood, infection, accidents, and cephalo-pelvic disproportion (CPD), the leading cause of primary cesarean section.
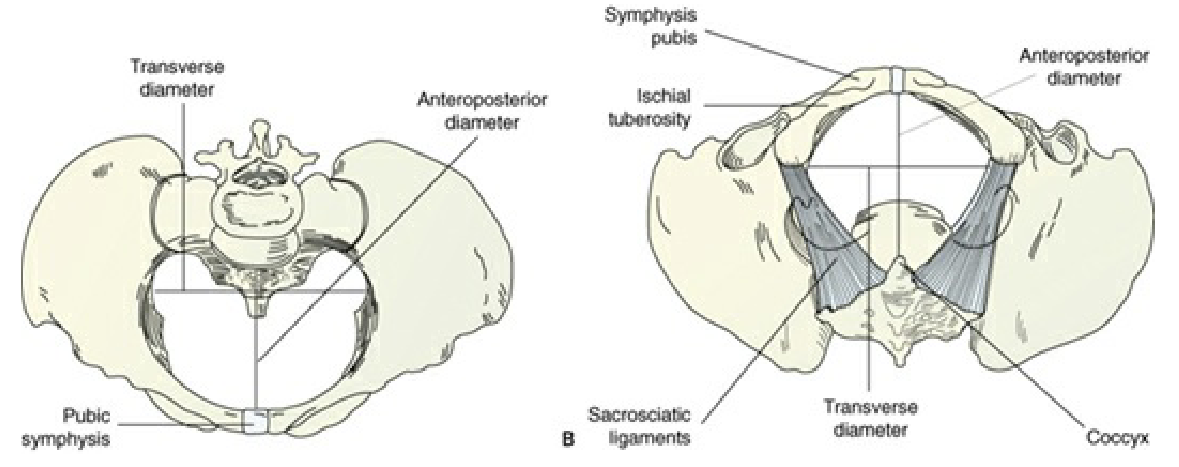
| Cavity | AP Diameter | Transverse | Oblique |
|---|---|---|---|
| Inlet | 11 cm | 13 cm | 12 cm |
| Cavity | 12 cm | 12 cm | 12 cm |
| Outlet | 13 cm | 11 cm | 12 cm |
Psyche
A pregnant woman’s general behavior and influences on her also affect labor progress. Some factors that make labor meaningful, positive or negative, even:
- Cultural influences integrating maternal attitudes; how a particular society views childbirth
- Expectations and goals for the labor process, whether realistic, achievable, or otherwise
- Feedback from other people participating in the birthing process.
This also includes the pregnant woman’s psychologic response to uterine contractions; fear and anxiety affect labor progress. A woman who is relaxed, aware of, and participating in the birth process usually has a shorter, less intensive labor.
Pain, and anticipation of pain can increase emotional tension and increase pain perception. Even though perceptions of childbirth pain are greatly influenced by a lot of factors, such as psychosocial factors, there is a physiologic basis for discomfort during labor.
- First Stage of Labor: distention and dilatation of the cervix is the primary source of pain in the first stage. Pain from the uterus is referred to as dermatoses supplied by the 12th, 11th, and 10th thoracic nerves, with referred pain to the lower abdominal wall and the areas over the lower lumbar region and upper sacrum. Thus, the characteristic sign of pain in true labor is lumbosacral radiating to the abdomen.
- Hypoxia of the uterine muscles during contraction also cause pain.
- Distension and stretching of the lower uterine segment in combination with isometric contraction of the uterus: if the fetus is large, there is more stretching of the lower uterine segment and more pressure on adjacent structures, causing more pain.
- Pressure on adjacent structures.
- Second Stage of Labor: tissue damage in the pelvis and perineum, ischemia/hypoxia of contracting uterine muscles, distention of the vagina and perineum, and pressure on adjacent structures.
- Distention of the vagina and perineum: the nerve impulses travel via the pudendal nerve plexus and enter the spinal cord through the posterior roots of the second, third, and fourth sacral nerves. As such, the pudendal block technique is employed, relieving pain from perineal distention (but not uterine contractions).
- Pressure on adjacent structures: the larger the passenger, the harder the compressing part (fetal occiput in occipitoposterior positions), and the longer the time of pressure on adjacent structures (prolonged contractions); thus, the more pain and discomfort is experienced by the parturient.
Other factors include:
- Childbirth preparation process (classes): considered a valuable tranquilizer during the birth process; could decrease the need for analgesics in labor.
- Support system: the husband’s (or companion of choice) presence in the labor and delivery unit, the nurse’s supportive and caring environment, and therapeutic communication all contribute to the support a mother receives during labor and delivery.
- Previous experiences