References:
- Wong’s Nursing Care of Infants and Children, 11th Edition, ISBN 978-0-323-54939-4, by Marilyn J. Hockenberry, David Wilson, and Cheryl C. Rodgers (Ch. 26, pp. 1091–1093)
- TRA Modules
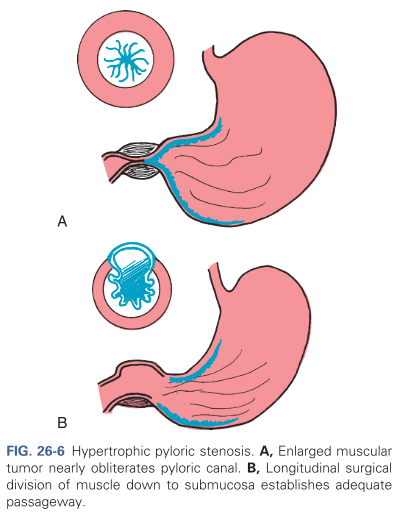
Hypertrophic pyloric stenosis (HPS) occurs when the circumferential muscle of the pyloric sphincter becomes thickened, resulting in elongation and narrowing of the pyloric canal. This produces an outlet obstruction and compensatory dilation, hypertrophy, and hyperperistalsis of the stomach. This condition usually develops in the first few weeks of life, causing nonbilous vomiting, which occurs after feeding; projectile vomiting may develop and the infant is fussy and hungry after vomiting.
- If undiagnosed, dehydration, metabolic alkalosis, and failure to thrive may occur.
- Precise etiology is unknown, but HPS is more common in boys by four to six times than in girls. It is also less common in African-American infants than Caucasian infants, and rare in Asians. Inheritance is polygenic, with an increased risk in the siblings and offspring of affected persons.
Pathophysiology
The circular muscle of the pylorus thickens as a result of hypertrophy. This produces severe narrowing of the pyloric canal between the stomach and the duodenum. Consequently, the lumen at this point is partially obstructed. Over time the size of the opening is reduced, and the partial obstruction may progress to complete obstruction.
- The hypertrophied pylorus may be palpable as an olive-like mass in the upper abdomen.
- Pyloric stenosis is not a congenital disorder. Evidence suggests that local innervation may be involved with the pathogenesis. In most cases, this is an isolated lesion; however, it may be associated with intestinal malrotation, esophageal and duodenal atresia, and anorectal abnormalities.
Clinical Manifestations
The infant will begin vomiting as early as 1 week and as late as 5 months, usually at 3 weeks of age. Vomiting episodes normally occur immediately after each feeding.
- Nonbilious vomiting, as the vomitus originates from the stomach, not reaching the duodenum where bile is deposited. Vomitus may become brown or blood-tinged if gastritis develops.
- Projectile vomiting may occur and appear progressively. Vomitus may reach as far as 3 to 4 feet if side-lying and 1 feet if back-lying.
- Prolonged vomiting may lead to dehydration, weight loss, and failure to thrive.
- Gastric peristalsis (left-to-right) may become visible during examination. The upper abdomen may also be visible distended.
- An olive-shaped mass in the epigastrium, just to the right of the umbilicus may be palpated.
- Indirect hyperbilirubinemia may be present in a small percentage of affected infants, reported occur as a result of a decreased level of glucuronyl transferase.
- The infant may display hunger; avid feeding even after vomiting. Other than chronic hunger, no pain or discomfort may be noted.
Diagnostic Evaluation
A diagnosis is often made after the history and physical examination.
- The olive-like mass is most easily palpated when the stomach is empty, the infant is quiet, and the abdominal muscles are relaxed.
- Ultrasonography can demonstrate an elongated mass surrounding a long pyloric canal. If this is not observed, GI radiography should be done to rule out other causes of vomiting.
- Laboratory findings can display fluid and electrolyte imbalances if the condition is not diagnosed early.
- Lowered sodium and potassium levels are present, but may be masked by proportional hemoconcentration.
- A greater diagnostic value is placed on chloride levels and a corresponding rise in pH and bicarbonate, indicative of metabolic alkalosis.
Therapeutic Management
The standard therapy instituted is a pyloromyotomy (pyloroplasty). Preoperatively, infants with evidence of fluid and electrolyte imbalances must be rehydrated and metabolic alkalosis must be corrected via parenteral fluid and electrolyte administration. This may delay surgery by 24 to 48 hours. NG tube decompression may be required for infants who continue to vomit.
A pyloromyotomy or the Fredet-Ramstedt operative procedure is a high-success procedure often performed via laparoscope that involves the creation of a longitudinal incision through the circular muscle fibers of the pylorus down to, but not including, the submucosa (refer to B in the image above)
Postoperatively, feedings may be continued within 4 to 6 hours, beginning with small, frequent feedings of water or electrolyte solutions. If these are retained, about 24 hours after surgery formula is started in the same small increments. The amount and the interval between feedings is gradually increased until a full feeding schedule is reinstated, which usually takes about 48 hours.
- Vomiting may continue to occur due to edema of the pylorus (~50% of infants). However, prolonged vomiting should be investigated further.
- Infants between 2 and 8 weeks of age may become apneic postoperatively due to CNS immaturity and anesthesia. Monitor closely for 24 hours prior to discharge.
Nursing Care Management
The nurse primarily observes for clinical features that help establish the diagnosis, careful regulation of fluid therapy, and reestablishment of normal feeding patterns.
- HPS should be considered a possibility in infants who fail to gain weight and has a history of vomiting after feedings. Assessment should be based on observation of eating behaviors, evidence of characteristic clinical manifestations, hydration, and nutritional status.
- Preoperatively, NPO is begun and IV of dextrose, sodium chloride, and added potassium may be indicated. The nurse should assess skin and mucous membrane status for alterations in hydration status.
- Infants who are receiving IV fluids may be given a pacifier to meet nonnutritive sucking needs.
- Stomach decompression and gastric lavage may be done. The nurse is responsible for ensuring NG patency, functioning, and documentation of drainage.
- Postoperatively, vomiting is not uncommon during the first 24 to 48 hours. Preoperative measures are continued, and IV fluids are administered until the infant is taking and retaining adequate amounts by mouth.
- Monitoring of vital signs, fluid status, and intake and output
- Appropriate analgesics around the clock
Provide support for the patients. Involve them in the care of the infant when necessary and reassure them that the condition was the result of a structural problem and that it is not a reflection of their parenting skills and capacities.
Feeding is instituted within several hours postoperatively, beginning with clear liquids. They are offered in small quantities at frequent intervals. If the infant has been breastfed, breast milk expressed by the mother may be given by bottle when the infant is able to tolerate feedings, or the mother is instructed to limit nursing time and gradually increase the time to previous patterns. Supervision of feedings is an important part of postoperative care.