References:
- Wong’s Nursing Care of Infants and Children, 11th Edition, ISBN 978-0-323-54939-4, by Marilyn J. Hockenberry, David Wilson, and Cheryl C. Rodgers (Ch. 25, pp. 860–861)
- Maternal & Child Health Nursing: Care of the childbearing & childrearing family, 8th Edition, ISBN 978-1-4963-4813-5, by JoAnne Silbert-Flagg and Adele Pillitteri (Ch. 45, pp. 2776–2778)
- Saunders Comprehensive Review for the NCLEX-RN Examination, 9th Edition, ISBN 978-032-37-9530-2, by Linda Anne Silvestri, Angela E. Silvestri, and Jessica Grimm (Ch. 34, pp. 433–434)
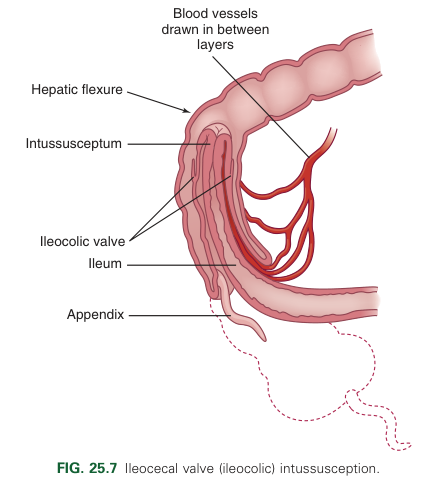
Intussusception occurs when a proximal segment of the bowel telescopes into a more distal segment, pulling the mesentery with it. The mesentery is compressed and angled, resulting in lymphatic and venous obstruction. As the edema from the obstruction increases, pressure within the area of intussusception increases. When this pressure matches arterial pressure, blood flow stops, resulting in ischemia and the pouring of mucus into the intestine. Venous engorgement also leads to leaking of blood and mucus into the intestinal lumen, forming the classic currant jelly-like stools. The most common site is the ileocecal valve (ileocolic) where the ileum invaginates into the cecum and then further into the colon. This may also be ileoileal or colocolic (usually in the area of the hepatic or splenic fixture or at some point along the transverse colon).
- Incidence: Intussusception is the most common cause of intestinal obstruction in children between 3 months and 6 years old, more common in children younger than 2 years old. It is more common in males than in females.
- Etiology: Only 12.5% to 25% of intussusception cases have a pathologic lead point (a lesion at the tip of the intussusceptum), such as a polyp, lymphoma, or Meckel diverticulum. Besides these cases, the cause is generally not known. The idiopathic cases may be caused by hypertrophy of intestinal lymphoid tissue secondary to viral infection.
- Clinical Manifestations: Intussusception usually manifests with the sudden onset of crampy abdominal pain, inconsolable crying, and a drawing up of the knees to the chest (as a result of a peristaltic wave) in an otherwise healthy child—symptom free and happy after the episode of pain. More specifically, this includes:
- Sudden acute abdominal pain
- Child screaming and drawing the knees onto the chest
- Child appearing normal and comfortable between episodes of pain
- Bilious vomiting and lethargy (as the obstruction progresses).
- Passage of red, currant jelly-like stools (stool mixed with blood and mucus)
- Tender, distended abdomen
- Palpable sausage-shaped mass in upper right quadrant
- Empty lower right quadrant—Dance’s sign—as the ileum moves upwards into the ascending colon.
- Eventual fever, prostration, abdominal guarding, leukocytosis, and often a rapid pulse, and other signs of peritonitis.
- Atypical Presentations: 30% or less of children present with the classic triad of intussusception—abdominal pain, abdominal mass, bloody stools. A more chronic case may be presented, characterized by diarrhea, anorexia, weight loss, occasional vomiting, and periodic pain. Atypical presentation may have lethargy as the primary symptom. If the distal bowel remains distended, necrosis and perforation are possible. Because intussusception is potentially life-threatening, awareness of such signs and prompt referral for further medical evaluation is important.
Diagnostic Evaluation
- Frequently, subjective findings and history lead to the diagnosis. Any time a parent is describing a child who is crying, be certain to ask enough questions to recognize the possibility of intussusception. Episodes of crying are for a short time but repeat every 15 to 20 minutes; the stomach feels “full” and vomitus and diarrhea with blood may occur.
- Definitive diagnosis may be made through ultrasonography or x-ray (and other imagine techniques) revealing a characteristic heterogenous mass and a “bull’s eye”, “target” or “donut” appearance (Radiopaedia).
- A rectal exam reveals mucus, blood, and occasionally a low intussusception itself.
Therapeutic Management
Nonoperative reduction is successful in the majority of stable cases. Gas enema is slightly more successful with reduction compared to a hydrostatic enema (83% versus 70%, respectively, 2017). Surgery is required for patients in whom the reduction is unsuccessful or for patients who are unstable. With early diagnosis and treatment, serious complications and death are uncommon.
- Pneumoenema (pneumatic insufflation), reduction performed with gas, is a conservative treatment done under the guidance of a radiologist. Recurrence of intussusception after conservative treatment is rare; however, this procedure should not be attempted with prolonged intussusception, signs of shock, peritoneal irritation, or intestinal perforation.
- IV fluids, nasogastric decompression, and antibiotic therapy may be used before hydrostatic reduction (water-soluble solution, barium enema) is attempted. If these procedures are not successful, the child may require surgical intervention.
- Surgery involves manually reducing the invagination and, when indicated, resecting any nonviable intestine.
Nursing Care Management
The nurse can help establish a diagnosis by listening to the parent’s description of the child’s physical and behavioral symptoms. The description of the child’s severe colicky abdominal pain combined with vomiting is a significant sign of intussusception.
- Parent education: It is important to explain the basic defect of intussusception. The nurse can easily demonstrate this by creating a model of the defect. Use the example of a telescoping rod, or push the end of a finger on a rubber glove back into itself. Then demonstrate the principle of reduction by hydrostatic pressure by filling the glove with water, which pushes the “finger” into a fully extended position.
- Preprocedural Care: Physical care of the child does not differ from that for any child undergoing abdominal surgery. Even though nonsurgical intervention may be successful, the usual preoperative procedures, such as maintenance of NPO status, routine laboratory testing (CBC and urinalysis), signed parental consent, and preanesthetic sedation, are performed.
- Monitor for signs of perforation or shock as these are contraindications to reduction by gas or fluid, which exerts pressure on the bowel.
- Children with perforation will require IV fluids, systemic antibiotics, and bowel decompression before undergoing surgery. Fluid volume replacement and restoration of electrolytes may be required in such children before surgery. Before surgery the nurse monitors all stools.
Spontaneous Reduction
Passage of a normal brown stool usually indicates that the intussusception has reduced itself. This is immediately reported to the practitioner, who may choose to alter the diagnostic and therapeutic care plan.
- Postprocedural Care: Postprocedural care includes observations of vital signs, blood pressure, intact sutures and dressing, and the return of bowel sounds. After spontaneous or hydrostatic reduction, the nurse observes for passage of water-soluble contrast material or barium (if used) and the stool patterns because the intussusception may recur. Children may be admitted to the hospital or monitored on an outpatient basis.
- Following a nonsurgical reduction, infants are kept NPO for a few hours and then introduced from clear fluids to regular feedings gradually as prescribed. Parents should be encouraged to participate to help regain confidence in themselves as parents.
- Infants who have surgery will return with a nasogastric tube attached to low intermittent suction and an IV infusion in place. The nasogastric tube will remain in place until the suture line is healing, and peristaltic function has returned.
- Observation for 24 hours is performed after hydrostatic or pneumatic reduction due to the possibility of recurrence.
- A recurrence of intussusception is treated with the conservative reduction techniques described previously, but a laparotomy is considered for multiple recurrences.
Nursing Diagnoses and Related Interventions
- Pain related to abnormal abdominal peristalsis
- Outcome evaluation: Child can be comforted between spasms of pain; demonstrates interest in toys or social interactions.
- Children are bewildered by this type of episodic pain. In other types of pain, the parent comforts the child and the pain goes away. With intussusception, the pain goes away then re-appears. They must be comforted in an attempt to relieve their fright at this strange happening.
- Risk for deficient fluid volume related to bowel obstruction
- Outcome evaluation: Infant’s skin turgor is good, pulse is 90 to 100 beats/min, amount of diarrhea and blood loss in stool are minimal; episodes of vomiting decrease in frequency.
- Infants are kept on NPO status before surgery or nonsurgical reduction. Because they have abdominal pain, they may find comfort in sucking a pacifier. Because they have been vomiting, IV fluid therapy may be started to reestablish their electrolyte balance and to supply adequate fluid to hydrate them.