References:
- Maternal & Child Health Nursing: Care of the childbearing & childrearing family, 8th Edition, ISBN 978-1-4963-4813-5, by JoAnne Silbert-Flagg and Adele Pillitteri (Unit 5, Growth and Development)
Assessing for growth and development milestones is a nursing role in the care of both well and ill children.
- Health Promotion and Illness Prevention: determining a child’s developmental stage is often the primary focus of a well-child health interview and examination. For instance, during her child’s 24-month checkup, a mother might ask if it is normal that her child cannot yet pedal a tricycle, a question that cannot be answered without a full understanding of average ranges of motor coordination.
- Health Restoration and Maintenance: it is equally essential to consider the developmental stage of a child when providing care during illness (both acute and chronic) and in preparation for a medical or surgical procedure. Preparing a 5-year-old child for surgery, for example, would be ineffective unless you know how much a 5-year-old child will understand (e.g., anesthesia, some body parts are necessary for life and some are not, or stitches will not stay in permanently). During the postsurgical period, you need growth and development knowledge to assess whether a child is old enough to swallow pills, whether a child will be able to accurately rate a degree of pain on a standard scale, and how to approach a child who says “no” to every suggestion.
Principles of Growth and Development
The terms “growth” and “development” are sometimes used interchangeably, but they are actually different terms.
- Growth is used to denote an increase in physical size or a quantitative change. Growth in weight, for example, is measured in pounds or kilograms; growth in height is measured in inches or centimeters.
- Development indicates an increase in skill or the ability to function (a qualitative change). Development is measured by observing a child’s ability to perform specific tasks such as how well a child picks up small objects, by recording the parent’s description of a child’s progress, or by using standardized tests such as the Metro Manila Developmental Screening Test.
- Psychosexual Development (Freud’s Theory) refers to developing instincts or sensual pleasure.
- Psychosocial Development (Erikson’s Theory) refers to Erikson’s stages of personality development.
- Moral Development (Kohlberg’s Theory) is the ability to know right from wrong and to apply these to real-life situations.
- Cognitive Development (Piaget’s Theory) refers to the ability to learn or understand from experience, to acquire and retain knowledge, to respond to a new situation, and to solve problems. It is measured by intelligence tests and by observing children’s ability to function effectively in different environments.
Patterns of Growth and Development
- Growth and development are continuous processes from conception until death. Although there are highs and lows in terms of the rate at which growth and development proceed, a child is growing new cells and learning new skills at all times.
- Growth and development proceed in an orderly sequence. Growth in height occurs in only one sequence—from smaller to larger. Development also proceeds in a predictable order. For example, the majority of children sit before they crawl, crawl before they stand, stand before they walk, and walk before they run.
- Children pass through the predictable stages at different rates. All stages of development have a range of time rather than a certain point at which they are usually accomplished.
- All body systems do not develop at the same rate. Certain body tissues mature more rapidly than others. For example, neurologic tissue experiences its peak 1656 growth during the first year of life, whereas genital tissue grows little until puberty.
- Development is cephalocaudal. Cephalo- is a Greek word meaning “head”; caudal means “tail.” Development proceeds from head to tail. Newborns can lift only their head off the bed when they lie in a prone position. By age 2 months, infants can lift both the head and chest off the bed; by 4 months, the head, chest, and part of the abdomen; by 5 months, infants have enough control to turn over; by 9 months, they can control legs enough to crawl; and by 1 year, children can stand upright and perhaps walk.
- Development proceeds from proximal to distal body parts. This principle is closely related to cephalocaudal development. It can best be illustrated by tracing the progress of upper extremity development. A newborn makes little use of the arms or hands. By age 3 or 4 months, the infant has enough arm control to support the upper body weight on the forearms, and can coordinate the hand to scoop up objects. By 10 months, the infant can coordinate the arm and thumb and index fingers sufficiently to use a pincerlike grasp or to be able to pick up an object as fine as a piece of breakfast cereal on a high chair tray.
- Development proceeds from gross to refined skills. This principle parallels the preceding one. Once children are able to control distal body parts such as fingers, they are able to perform fine motor skills (e.g., a 3-year-old colors best with a large crayon; a 12-year-old can write with a fine pen).
- There is an optimum time for initiation of experiences or learning. Children cannot learn tasks until their nervous system is mature enough to allow that particular learning. A child cannot learn to sit, for example, no matter how much the child’s parents have him or her practice, until the nervous system has matured enough to allow for back control.
- Neonatal reflexes must be lost before development can proceed. An infant cannot grasp an item with skill until the grasp reflex has faded nor can the infant stand steadily until the walking reflex has faded. Neonatal reflexes are replaced by purposeful movements.
Factors Influencing Growth and Development
Genetic and environmental influences are primary factors in determining if a child will be able to reach his or her genetic potential. Temperament—the typical way a child reacts to situations—is an example of genetic influence.
- Genetics: from the moment of conception when a sperm and ovum fuse, the basic genetic makeup of an individual is cast. In addition to physical characteristics such as eye color and height potential, inheritance determines characteristics such as learning style. A child may also inherit a genetic abnormality, which could result in disability or illness at birth or later in life and so prevent optimal growth.
- Gender: on average, girls are born lighter (by an ounce or two) and shorter (by an inch or two) than boys. Boys tend to keep this height and weight advantage until prepuberty, at which time girls surge ahead as they begin their puberty growth spurt 6 months to 1 year earlier than boys. By the end of puberty (age 14 to 16 years), boys again tend to be taller and heavier than girls.
- Health: a child who inherits a genetically transmitted disease may not grow as rapidly or develop as fully as a healthy child depending on the type of illness and the therapy or care available for the disease.
- Intelligence: children with high intelligence do not generally grow faster physically than other children, but they do tend to advance faster in skills. Occasionally, children of high intelligence actually fall behind in physical skills because they spend their time with books or mental games rather than with games that develop motor skills.
- Temperament: temperament is the usual reaction pattern of an individual or an individual’s characteristic manner of thinking, behaving, or reacting to stimuli in the environment. Unlike cognitive or moral development, temperament is not developed in stages but is an inborn characteristic set at birth.
Reaction Patterns
There are nine separate characteristics that define temperament (Chess and Thomas, 1985): activity level, rhythmicity (time of waking, nap time, bowel movement, etc.), approach (response on initial contact to a new stimulus), adaptability (change in one’s reaction to stimuli over time), intensity of reaction, distractibility, attention span and persistence, threshold of response (level of intensity required to evoke a reaction), mood quality (positive—always happy and laughing, or negative) Based on temperament, children can be classified as:
- The Easy Child, easy to care for with predictable rhythmicity, approaches and adapts to new situations readily, mild-to-moderate intensity, and overall positive mood quality. Most children are rated by their parents as being in this category.
- The Intermediate Child, a mix between the easy child and the difficult child
- The Difficult Child, making up about 10% of children, exhibit irregular habits, negative mood quality, and withdraws rather than approaches new situations.
- The Slow-to-Warm-Up Child who stays fairly inactive and adapt slowly to new situations, and has a general negative mood.
- Environment: although children cannot grow taller than their genetically programmed height potential allows, their adult height can be considerably less than their genetic potential if their environment hinders their growth.
- Socioeconomic Level. Because health care and good nutrition both cost money, children born into families of low socioeconomic means may suffer from a lack of both of these.
- Parent-Child Relationship. What a parent expects a child to become as an adult varies from culture to culture and family to family but plays a role in how much a child is guided to try to achieve in life. Children who are loved and are paid attention to by their parents thrive better than those who are not. Luckily, for parents and children, either parent or even a nonparent may form this primary parent–child love relationship.
- Ordinal Position in the Family. The position of a child in the family (e.g., first-born child, middle child, youngest child, only child) and the size of the family. An only child or the oldest child in a family, for example, generally excels in language development because conversations are mainly with adults. Youngest children, in contrast, may develop language more slowly, especially if older children talk “baby talk” with them. Children learn by watching other children, however, so a youngest child who has many examples to watch may excel in other skills, such as toilet training or writing at an early age.
- Health. Diseases that come from environmental sources can have as strong an influence on growth and development as genetically inherited diseases.
- Nutrition. Poor maternal nutrition may limit the growth and intelligence potential of a child by furnishing a less than desired prenatal environment. In some communities, poor nutrition has such an effect that children begin to show inadequate physical growth as early as infancy. A lack of energy and stamina prevents children from learning at their best intellectual level, which causes them to fall behind in school. Children who become obese may develop motor skills more slowly than other children because physical movement is more tiring for them.
Theories of Child Development
Developmental theories are theories that provide road maps for explaining human development. Developmental tasks are a skill or a growth responsibility arising at a particular time in an individual’s life, the achievement of which will provide a foundation for the accomplishment of future tasks. However, for reference, childhood is generally divided into seven age periods:
| Stage | Age Period |
|---|---|
| Neonate | First 28 days of life |
| Infant | 1 month–1 year |
| Toddler | 1–3 years |
| Preschooler | 3–5 years |
| School-age child | 6–12 years |
| Adolescent | 13–17 years |
| Late adolescent | 18–21 years |
Freud’s Psychoanalytic Theory based on Freud’s observations of mentally disturbed adults, described adult behavior as being the result of instinctual drives of a primarily sexual nature (libido). He described child development as being a series of psychosexual stages in which a child’s sexual gratification becomes focused on a particular body part at each stage.
| Psychosexual Stage | Description | Nursing Implications |
|---|---|---|
| Infant: Oral stage | Child explores the world by using the mouth. | Provide oral stimulation by giving pacifiers; do not discourage thumb sucking. |
| Toddler: Anal stage | Child learns to control urination and defecation. | Help children achieve bowel and bladder control without undue emphasis on its importance. |
| Preschooler: Phallic stage | Child learns sexual identity through awareness of genital area. | Accept children’s sexual interest, such as fondling his or her own genitals, as a normal area of exploration. |
| School-age child: Latent stage | Child’s personality development appears to be nonactive or dormant. | Help children have positive experiences with learning so their self esteem continues to grow. |
| Adolescent: Genital stage | Adolescent develops sexual maturity and learns to establish satisfactory relationships with others. | Provide appropriate opportunities for the child to relate with opposite and own sex relationships. |
Erikson’s Theory of Psychosocial Development stresses the importance of culture and society in development of the personality. One of the main tenets of his theory, that a person’s social view of self is more important than instinctual drives in determining behavior, allows for a more optimistic view of the possibilities for human growth. Whereas Freud looked at ways mental illnesses develop, Erikson looked at actions that lead to mental health. He describes eight developmental stages covering the entire life span. At each stage, there is a conflict between two opposing forces. The resolution of each conflict, or accomplishment of the developmental task of that stage, allows the individual to go on to the next phase of development.
- The Infant: “learning confidence” or “learning to love”. When an infant is hungry, wet, or cold, a parent feeds, changes, or holds the baby closely and makes the infant comfortable again. By these simple processes, infants learn to trust that when they have a need or are in distress, a parent will come and meet that need.
- If care is inconsistent, inadequate, or rejecting, infants learn mistrust; they become fearful and suspicious of people and then of the world.
- The Toddler: self-governance or independence. These arise from a toddler’s new motor and mental abilities. Children take pride in new things they can accomplish and wish to do everything independently. When infants approach toddlerhood, they begin to make the differentiation between one’s body and others. As they recognize they are separate individuals, toddlers also realize they do not always have to do what others want them to do. From this realization comes the reputation toddlers have for being negativistic, obstinate, and difficult to manage.
- Children who are constantly told not to try things because they will hurt themselves may be left with a stronger sense of doubt than confidence at the end of the toddler period. Children who are made to feel it is wrong to be independent may leave the toddler period with a stronger sense of shame than autonomy.
- The Preschooler: learning how to do things such as drawing, building an object from blocks, or playing dress up. Children initiate motor activities of various sorts on their own or no longer merely respond to or imitate the actions of other children or their parents. The same is true for language and fantasy activities. Whether children leave this stage with a sense of initiative outweighing a sense of guilt depends largely on how parents respond to self-initiated activities. When children are given much freedom and opportunity to initiate motor play such as running, bike riding, sliding, and wrestling or are exposed to such play materials as finger paints, sand, water, and modeling clay, their sense of initiative is reinforced. Initiative is also encouraged when parents answer a child’s questions (intellectual initiative) and do not inhibit fantasy or play activity.
- In contrast, if children are made to feel their motor activity is bad (perhaps in a small apartment or in a hospital), their questions are a nuisance, or their play is silly, they can develop a sense of guilt over self-initiated activities that will persist in later life. Those who do not develop initiative have limited brainstorming and problem-solving skills later in life; instead, they wait for clues or guidance from others before acting.
- The School-age Child: self-confidence rather than inferiority. During the preschool period, children learned initiative (i.e., how to do things). During school age, children learn how to do things well. When they are encouraged in their efforts to do practical tasks or make practical things and are praised and rewarded for the finished results, their sense of industry grows.
- Parents who see their children’s efforts at making and doing things as merely “busy work” or who do not show appreciation for their children’s efforts may cause them to develop a sense of inferiority rather than pride and accomplishment.
- The Adolescent: adolescents must bring together everything they have learned about themselves as a son or daughter, an athlete, a friend, a fast-food cook, a student, a garage band musician, and so on, and integrate these different images into a whole that makes sense.
- Some adolescents may seek a negative identity: being identified as a drug abuser or runaway is not a positive identification but may be preferable to seemingly having no identity at all. Body piercing and tattooing are ways adolescents can help establish their identity because they are outward expressions of who adolescents think they are.
- The Late Adolescent: intimacy versus isolation. Intimacy is the ability to relate well with other people in preparation for developing future relationships. It grows out of earlier developmental tasks because people need a strong sense of identity before they can reach out fully and offer deep friendship or love to others.
- Because there is always the risk of being rejected or hurt when offering love or friendship, individuals cannot offer it if they do not have confidence that they can cope with rejection or if they did not develop a sense of trust as an infant or autonomy as a toddler. This is important for maternal and child health nursing because parents without a sense of intimacy may have more difficulty than others accepting a pregnancy and beginning to love a new child.
| Psychosocial Stage | Description | Nursing Implications |
|---|---|---|
| Infant: Oral stage | Developmental task is to form a sense of trust versus mistrust. Child learns to love and be loved. | Provide a primary caregiver. Provide experiences that add to security. |
| Toddler: Anal stage | Developmental task is to form a sense of autonomy versus shame. Child learns to be independent and make decisions for self. | Provide opportunities for independent decision making, such as choosing own clothes. |
| Preschooler: Phallic stage | Developmental task is to form a sense of initiative versus guilt. Child learns how to do things (basic problem solving) and that doing things is desirable. | Provide opportunities for exploring new places or activities. Allow free-form play. |
| School-age child: Latent stage | Developmental task is to form a sense of industry versus inferiority. Child learns how to do things well. | Provide opportunities such as allowing child to assemble and complete a short project. |
| Adolescent: Genital stage | Developmental task is to form a sense of identity versus role confusion. Adolescents learn who they are and what kind of person they will be. | Provide opportunities for an adolescent to discuss feelings about events important to him or her. Offer support and praise for decision making. |
Piaget’s Theory of Cognitive Development has roots similar to those of both Freud and Erikson, but with differing aspects. Piaget defined four stages of cognitive development, within the stages of growth, then finer units or schemas. To progress from one period to the next, children reorganize their thinking processes to bring them closer to adult thinking.
- The Infant: sensorimotor intelligence is practical intelligence because an infant is not yet able to use words and symbols for thinking and problem solving at this early age. At the beginning of life, babies relate to the world through their senses, using only reflex behavior. During this stage, infants learn objects in the environment—their bottle, blocks, their bed, or even a parent—are permanent and continue to exist even though they are out of sight or changed in some way. The world begins to make sense and the developmental task of achieving trust falls into place when the concept of permanence has been learned (i.e., infants know their parents exist and will return to them). Gaining a concept of permanence also contributes to separation anxiety, which can begin between 8 and 12 months of age.
- Infants identify that they are a separate entity from objects. They learn where their body stops and their bed, playthings, or parent begins.
- Infants are only ready to play peek-a-boo when they’ve mastered permanence because only then do they realize the person playing with them exists behind his or her hands.
- The Toddler: this stage completes the fifth and sixth stages of the sensorimotor period and begin to develop some cognitive skills of the preoperative period, such as symbolic thought and egocentric thinking. They complete their understanding of object permanence, begin to use symbols to represent objects, and start to draw conclusions from obvious facts that they see.
- The Preschooler: Preschool children move on to a substage of preoperational thought termed intuitive thinking. During this period, when young children look at an object, they are able to see only one of its characteristics. For example, they see a banana is yellow but do not notice that it is also long. Intuitive thinking is noticeable when children are learning about medicine (they observe it tastes bitter but cannot understand it is also good for them).
- Egocentric (unable to see the viewpoint of another).
- Static thinking (inability to remember what they started talking about so at the end of a sentence children are talking about another topic).
- Concept of time is “now”.
- Concept of distance is only as far as they can see.
- Centering (focusing on a single aspect of an object) causes distorted reasoning.
- No awareness of reversibility is present.
- Unable to state cause-effect relationships, categories, or abstractions.
- The School-age Child: Piaget viewed school age as a period during which concrete operational thought begins because school-age children can be seen using practical solutions to everyday problems as well as begin to recognize cause-and-effect relationships.
- Child is aware of reversibility, where operations or steps are taken in reverse to return to a starting point.
- Understands conservation, sees constancy despite transformation (mass or quantity remains the same even if it changes shape or position).
- The Adolescent: the time when cognition achieves its final form or when formal operational thought begins. When this stage is reached, adolescents are capable of thinking in terms of possibility—what could be (abstract thought)—rather than being limited to thinking about what already is (concrete thought). This makes it possible for adolescents to use scientific reasoning. They can use deductive reasoning in addition to the induction reasoning they used during school age or can move from the general to the specific (e.g., plastic toys break easily, the toy they are holding is plastic; therefore, it will break easily).
| Stage of Development | Age Span | Nursing Implications | Activities |
|---|---|---|---|
| Neonatal Reflex | 1 month | Stimuli are assimilated into beginning mental images. Behavior entirely reflexive. | N/A |
| Primary Circular Reaction | 1–4 months | Hand–mouth and ear–eye coordination develop. | Enjoyable activity for this period: a rattle or tape of parent’s voice. |
| Secondary Circular Reaction | 4–8 months | Infant learns to initiate, recognize, and repeat pleasurable experiences from environment. | Good toy for this period: mirror; good game: peek-a-boo. |
| Coordination of Secondary Reactions | 8–12 months | Infant can plan activities to attain specific goals. | Good toy for this period: nesting toys (i.e., colored boxes). |
| Tertiary Circular Reaction | 12–18 months | Child is able to experiment to discover new properties of objects and events. | Good game for this period: throw and retrieve. |
| Invention of new means through mental combinations | 18–24 months | Transitional phase to the preoperational thought period. | Good toys for this period: those with several uses, such as blocks or colored plastic rings. |
| Preoperational Thought | 2–7 years | Thought becomes more symbolic; can arrive at answers mentally instead of through physical attempt. Comprehends simple abstractions but thinking is basically concrete and literal. | Good toy for this period: items that require imagination, such as modeling clay. |
| Concrete Operational Thought | 7–12 years | Concrete operations includes systematic reasoning. Uses memory to learn broad concepts (fruit) and subgroups of concepts (apples, oranges). These elements are classified and serialized (ordered according to some characteristic). | Good activity for this period: collecting and classifying natural objects such as native plants or sea shells. Expose child to other viewpoints by asking questions such as, “How do you think you’d feel if you were a nurse and had to tell a boy to stay in bed?” |
| Formal Operational Thought | 12 years | Can solve hypothetical problems with scientific reasoning. | Good activity for this period: “talk time” to sort through attitudes and opinions. |
Kohlberg’s Theory of Moral Development studied the reasoning ability of boys and, based on Piaget’s development stages, developed a theory on the way children gain knowledge of right and wrong or moral reasoning.
| Age (in years) | Stage | Description | Nursing Implications |
|---|---|---|---|
| Preconventional (Level I) | |||
| 2–3 | 1 | Punishment/obedience orientation (“heteronymous morality”). Child does right because a parent tells him or her to and to avoid punishment. | Child needs help to determine what are right actions. Give clear instructions to avoid confusion. |
| 4–7 | 2 | Individualism. Instrumental purpose and exchange. Carries out actions to satisfy own needs rather than society’s. Will do something for another if that person does something for him or her. | Child is unable to recognize that like situations require like actions. Unable to take responsibility for self-care because meeting own needs interferes with this. |
| Conventional (Level II) | |||
| 7–10 | 3 | Orientation to interpersonal relations of mutuality. Child follows rules because of a need to be a good person in own eyes and eyes of others. | Child enjoys helping others because this is nice behavior. Allow child to help with bed making and other such activities. Praise for desired behavior such as sharing. |
| 10–12 | 4 | Maintenance of social order, fixed rules, and authority. Child finds following rules satisfying. Follows rules of authority figures as well as parents in an effort to keep the system working. | Child often asks what the rules are and if something is right. May have difficulty modifying a procedure because one method may not be right. Follows self care measures only if someone is there to enforce them. |
| Postconventional (Level III) | |||
| Older than 12 | 5 | Social contract, utilitarian law-making perspectives. Follows standards of society for the good of all people. | Adolescents can be responsible for self-care because they view this as a standard of adult behavior. |
| Older than 12 | 6 | Universal ethical principle orientation. Follows internalized standards of conduct. | Many adults do not reach this level of moral development. |
Nursing Care of a Family with an Infant
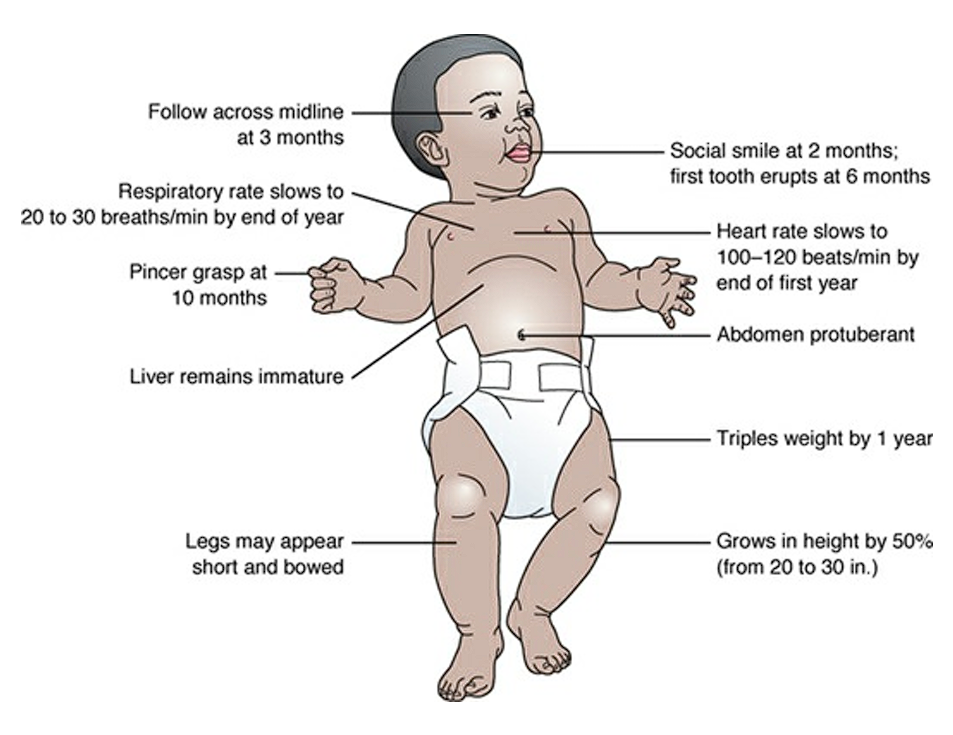
Traditionally, infancy is designated as the period of time from 1 month to 1 year of age. In these important months, an infant undergoes such rapid development that parents sometimes believe their baby looks different and demonstrates new abilities every day. During this time, an infant typically triples birth weight and increases length by 50%. Babies’ senses sharpen, and with the process of attachment to a primary caregiver, they form a first social relationship. Because of the growth and learning potential that occurs, this first year is a crucial one. Without proper nutrition, a baby will not grow and physically thrive; without proper stimulation and nurturing care by a consistent caregiver, an infant may not develop a healthy interest in life or a feeling of security essential for future development.
Physical Growth
- Weight: as a rule, most infants double their birth weight by 4 to 6 months and triple it by 1 year. On average, a weight gain of 2 lb. per month occurs during the first 6 months, then 1 lb. per month for during the second 6 months. However, the best measure of growth is with a standard growth chart.
- Height: An infant increases in height during the first year by 50%, or grows from the average birth length of 20 in. to about 30 in. (50.8 to 76.2 cm). Height, like weight, is best assessed if it is plotted on a standard growth chart.
- Head Circumference: By the end of the first year, the brain already reaches two thirds of its adult size. Head circumference increases rapidly during the infant period to reflect this rapid brain growth.
- Some infants’ heads appear asymmetric until the second half of the first year, especially if they are always placed on their back to sleep (which they should be), causing the skull bones to flatten in the back. Suggest to parents they continue to place the infant on the back to sleep but to spend “tummy time” daily with the infant placed in a prone position to prevent this flattening. Persistence of asymmetry suggests an infant is not receiving enough stimulation or is spending the majority of time lying in bed.
- Body Proportion:
- By the end of the infant period, the lower jaw is definitely prominent and remains that way throughout life.
- The circumference of the chest is generally less than that of the head at birth by about 2 cm. It is even with the head circumference in some infants as early as 6 months and in most by 12 months.
- The abdomen remains protuberant until the child has been walking well for some time, generally well into the toddler period. Cervical, thoracic, and lumbar vertebral curves develop as infants hold up their head, sit, and walk.
- Lengthening of the lower extremities during the last 6 months of infancy readies the child for walking and often is the final growth that changes the appearance from “babylike” to “toddlerlike.”
- Body Systems:
- In the cardiovascular system, heart rate slows from 110 to 160 beats/min to 100 to 120 beats/min by the end of the first year. The heart continues to occupy a little over half the width of the chest. Pulse rate may slow with inhalation (sinus arrhythmia), but this does not become marked until preschool age. That the heart is becoming more efficient is shown by a decreasing pulse rate and a slightly elevated blood pressure (from an average of 80/40 to 100/60 mmHg).
- Infants are prone to develop a physiologic anemia at 2 to 3 months of age. This occurs because the life of a typical red cell is 4 months, so the cells the child had at birth begin to disintegrate at that time, yet new cells are not yet being produced in adequate replacement numbers. Hemoglobin in an infant becomes totally converted from fetal to adult hemoglobin at 5 to 6 months of age. Infants may experience a decrease in serum iron levels at 6 to 9 months as the last of iron stores established in utero are used.
- The respiratory rate of an infant slows from 30 to 60 breaths/min to 20 to 30 breaths/min by the end of the first year. Because the lumens of the respiratory tract remain small and mucus production by the tract to clear invading microorganisms is still inefficient, upper respiratory infections occur readily and tend to be more severe than in adults.
- At birth, the gastrointestinal tract is immature in its ability to digest food and mechanically move it along. These functions mature gradually during the infant year. Although the ability to digest protein is present and effective at birth, the amount of amylase, which is necessary for the digestion of complex carbohydrates, is deficient until approximately the third month. Lipase, necessary for the digestion of saturated fat, is decreased in amount during the entire first year.
- The liver of an infant remains immature, possibly causing an inadequate conjugation of drugs (if a drug should be necessary for treatment of illness) and the inefficient formation of carbohydrate, protein, and vitamins for storage. Until age 3 or 4 months, an extrusion reflex (food placed on an infant’s tongue is thrust forward and out of the mouth) prevents some infants from eating effectively if they are offered solid food this early (not recommended). Newborns can drink from a cup as long as a parent controls the fluid flow. An infant can independently drink from a cup by age 8 or 10 months.
- The kidneys remain immature and not as efficient at eliminating body wastes as in an adult. The endocrine system remains particularly immature in response to pituitary stimulation, such as adrenocorticotropic hormone, or insulin production from the pancreas. Without these hormones functioning effectively, an infant may not be able to respond to stress as effectively as an adult.
- An infant’s immune system becomes functional by at least 2 months of age; an infant can actively produce both immune globulin (Ig)G and IgM antibodies by 1 year. The levels of other immunoglobulins (IgA, IgE, and IgD) are not plentiful until preschool age, which is the reason why infants continue to need protection from infection.
- The ability to adjust to cold is mature by age 6 months. By this age, an infant can shiver in response to cold (which increases muscle activity and provides warmth) and has developed additional adipose tissue to serve as insulation. The amount of brown fat, which protected the newborn from cold, decreases during the first year as subcutaneous fat increases.
- Although the fluid in body compartments shifts to some extent, extracellular fluid accounts for approximately 35% of an infant’s body weight, with intracellular fluid accounting for approximately 40% by the end of the first year, in contrast to adult proportions of 20% and 40%, respectively. This proportional difference increases an infant’s susceptibility to dehydration from illnesses, such as diarrhea, because loss of extracellular fluid could result in loss of over a third of an infant’s body fluid.
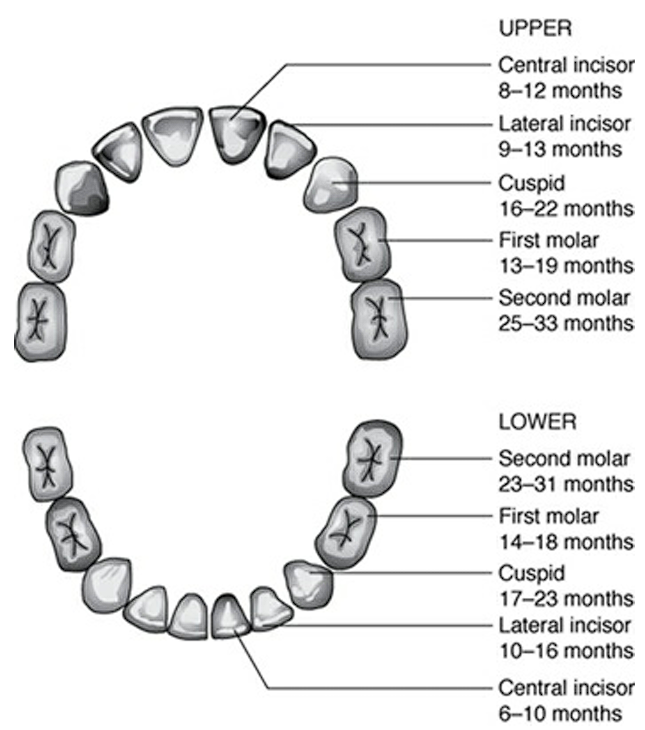
- Teeth: The first baby tooth (typically a central incisor) usually erupts at age 6 months, followed by a new one monthly. Fluoride supplementation should be administered at 6 months of age. However, teething patterns can vary greatly among children.
Motor Development
An average infant progresses through systematic motor growth during the first year, strongly reflecting the principles of cephalocaudal (head to toe) and gross-to-fine motor development. Control proceeds from head to trunk to lower extremities in a progressive, predictable sequence. As different infants show individual variations in accomplishing different tasks, the ages given here are only averages.
Gross Motor Development
Gross motor development (ability to accomplish large body movements) is assessed via four positions: ventral suspension, prone, sitting, and standing.
- Ventral Suspension Position: an infant’s appearance when held in midair on a horizontal plane and supported by a hand under the abdomen. In this position, the newborn allows the head to hang down with little effort at control.
- 1-month-old: head is below the plane of the body in ventral suspension
- 2-month-old: head is in line with the plane of the body in ventral suspension
- 3-month-old: head is above the plane of the body in ventral suspension. At this age, as the head is above the body, the Landau reflex develops. While held in the same position, the infant’s head, legs, and spine are extended. However, when the head is depressed by an examiner, the hips, knees, and elbows flex. This reflex is important because children with motor weakness, cerebral palsy, or other neuromuscular defects will not be able to demonstrate the reflex.
- 6- to 9-month-old: the parachute reaction from a ventral suspension position appears. This means that when infants are suddenly lowered toward an examining table, the arms extend as if to protect themselves from falling. Children with cerebral palsy do not demonstrate this response because they flex their extremities too tightly.

- Prone Position:
- Newborn: when lying on their stomach, newborns can turn their head to move it out of a position where breathing is impaired, but they cannot hold their head raised for an extended time.
- 1-month-old: By 1 month of age, they lift their head and turn it easily to the side.
- 2-month-old: Two-month-old infants can raise their head and maintain the position, but they cannot raise their chest high enough to look around yet. Their head is still held facing downward.
- 3-month-old: A 3-month-old child lifts the head and shoulders well off the table and looks around when prone. Some children can turn from a prone to a side-lying position at this age.
- 4-month-old: Four-month-old infants lift their chests off the bed and look around actively, turning their head from side to side. They are able to turn from front to back. The first time, this tends to occur as an extension of lifting the chest combined with a neck-righting reflex, which begins at this age. This reflex causes babies to lose their balance and roll sideways when lifting the head up. The baby is frightened by the sudden feeling of rolling free and probably cries. After this happens a few more times, however, a baby begins to delight in this new accomplishment.
- 5-month-old: Five-month-old infants are able to rest weight on their forearms when prone. They can turn completely over, front to back and back to front.
- 6-month-old: By 6 months, infants can raise their chests and the upper part of their abdomens off the table.
- 9-month-old: By 9 months, a child can creep from the prone position. Creeping means the child has the abdomen off the floor and moves one hand and one leg and then the other hand and leg, using the knees on the floor to locomote.

- Sitting: When placed on his or her back and then pulled to a sitting position, a newborn has extreme head lag; this lag is present until about 1 month. In a sitting position, the back appears rounded and an infant demonstrates only momentary head control.
- 2-month-old: By 2 months, infants can hold their head fairly steady when sitting up, although their head does tend to bob forward and will still show head lag when pulled to a sitting position.
- 4-month-old: A 4-month-old child reaches an important milestone by no longer demonstrating head lag when pulled to a sitting position.
- 5-month-old: A 5-month-old infant can be seen to straighten his or her back when held or propped in a sitting position.
- 6-month-old: By 6 months, infants can sit momentarily without support. They anticipate being picked up and reach up with their hands from this position.
- 7-month-old: A 7-month-old child can sit alone but only when the hands are held forward for balance.
- 8-month-old: An 8-month-old child can sit securely without any additional support. This is a major milestone in development that should always be considered in an assessment.
- 9-month-old: At 9 months, infants sit so steadily that they can lean forward and regain their balance. They may still lose their balance if they lean sideways, which is a skill not achieved for another month.
- Standing:
- Newborn: presence of the newborn stepping reflex, which may still be demonstrated by 1 month of age. In a standing position, the infant’s knees and hips flex rather than support more than momentary weight.
- 3-month-old: the infant tries to support part of their weight on their feet.
- 4-month-old: infants are able to support their weight on their legs, successful partly due to the faded stepping reflex.
- 5-month-old: the tonic neck reflex should be extinguished, and the Moro reflex fading.
- 6-month-old: By 6 months, infants nearly support their full weight when in a standing position.
- 7-month-old: A 7-month-old child bounces with enjoyment in a standing position.
- 9-month-old: Nine-month-olds can stand holding onto a coffee table if they are placed in that position.
- 10-month-old: Ten-month-olds can pull themselves to a standing position by holding onto the side of a playpen or a low table, but they cannot let themselves down again as yet.
- 11-month-old: At around 11 months, an infant learns to “cruise” or move about the crib or room by holding onto objects such as the crib rails, chairs, walls, and low tables.
- 12-month-old: At 12 months, the child can stand alone at least momentarily. Some parents expect children to walk at this time and may be disappointed to see their child is merely standing still. A child has until about 22 months of age to walk and still be within the normal limit, however. Typically, the age in which children can take their first step ranges from 8 to 15 months.

Fine Motor Development
Fine Motor Development is measured by observing or testing prehensile ability—ability to coordinate hand movements.
- 1-month-old: One-month-old infants still have a strong grasp reflex so they hold their hands in fists so tightly that it is difficult to extend their fingers.
- 2-month-old: As the grasp reflex fades, a 2-month-old infant will hold an object for a few minutes before dropping it. The hands are held open, not closed in fists.
- 3-month-old: By 3 months, infants reach for attractive objects in front of them. Their grasp is unpracticed so they usually miss them. You can assure parents this is part of normal development so they do not think their child is nearsighted or farsighted or has poor coordination.
- 4-month-old: When they reach 4 months, infants bring their hands together and pull at their clothes. They will shake a rattle placed in their hand. Thumb opposition (ability to bring the thumb and fingers together) begins, but the motion is a scooping or raking one, not a picking-up one, and is not very accurate. This limits the infant to handling large objects. Palmar and plantar grasp reflexes have disappeared.
- 5-month-old: Five-month-old children can accept objects that are handed to them by grasping with the whole hand. They can reach and pick up objects without the object being offered and often play with their toes as objects. Fisting that persists beyond 5 months suggests a delay in motor development. Unilateral fisting suggests hemiparesis or paralysis on that side.
- 6-month-old: By 6 months, grasping has advanced to a point where a child can hold objects in both hands. Infants at this age will drop one toy when a second one is offered, however. They can hold a spoon and start to feed themselves (with much spilling). The Moro, the palmar grasp, and the tonic neck reflexes have completely faded. A Moro reflex that persists beyond this point should arouse suspicion of neurologic disease.
- 7-month-old: Seven-month-old infants can transfer toys from one hand to the other. They hold a first object when a second one is offered.
- 8-month-old: By 8 months, random reaching and ineffective grasping disappear as a result of advanced eye–hand coordination.
- 10-month-old: A major milestone at 10 months is the ability to bring the thumb and first finger together in a pincer grasp (Fig. 29.10). This enables children to pick up small objects such as crumbs or pieces of cereal from a high chair tray. They use one finger to point to objects. They offer toys to people but then cannot release them.
- 12-month-old: At 12 months, infants can hold a crayon well enough to draw a semi-straight line. They enjoy putting objects such as small blocks in containers and taking them out again. They can hold a cup and spoon to feed themselves fairly well (if they have been allowed to practice) and can take off socks and push their hands into sleeves (again, if they have been allowed to practice). They can offer toys and release them.
Language Development
- 1-month-old: Infants begin to make small, cooing (dovelike) sounds by the end of the first month.
- 2-month-old: By 2 months, they can differentiate their cry. For example, parents can begin to distinguish a cry that means “hungry” from one that means “wet” or from one that means “lonely.” This is an important milestone in development for an infant; asking if a parent can tell the difference in crying is a good way to assess how far a parent has progressed in the task of parenting.
- 3-month-old: In response to a nodding, smiling face, or a friendly tone of voice, a 3-month-old infant will squeal with pleasure or laugh out loud. The same as with differentiating a cry, this is an important step in development because it makes a baby even more fun to be with. Parents spend increased time with infants at this age, not just to care for them but because they enjoy watching them smile at attention.
- 4-month-old: By 4 months, infants are very talkative, cooing, babbling, and gurgling when spoken to. They definitely laugh out loud.
- 5-month-old: By 5 months, an infant says some simple vowel sounds (e.g., “goo-goo,” “gah-gah”).
- 6-month-old: At 6 months, infants learn the art of imitating. They may imitate a parent’s cough, for example, or say “Oh!” as a way of attracting attention.
- 8-month-old: The amount of talking infants do increases still more at 7 months. They can imitate vowel sounds well (e.g., “oh-oh,” “ah-ah,” “oo-oo”).
- 9-month-old: By 9 months, an infant usually speaks a first word: “da-da” or “ba ba.” Occasionally, a mother may need reassurance that “da-da” for daddy is an easier syllable to pronounce than “ma-ma” for mommy. German mothers report the first word their babies say is “here,” which is “da” in German.
- 10-month-old: By 10 months, an infant masters another word such as “bye-bye” or “no.”
- 12-month-old: By 12 months, infants can generally say two words in addition to “ma-ma” and “da-da,” and they use those two words with meaning.
Play
- 1-month-old: Because 1-month-olds can fix their eyes on an object, they are interested in watching a mobile over their crib or playpen. Mobiles are best if they are black and white or brightly colored and light enough in weight so they move when someone walks by. Be sure they face down toward the infant, not toward the adult standing beside the crib. Musical mobiles provide extra stimulation. One-month-old children also spend a great deal of time watching their parents’ faces, appearing to enjoy this activity so much a face may become their favorite toy.
- 2-month-old: Hearing is a second sense that is a source of pleasure for children in early infancy. Even newborns listen to the sound of a music box or a musical rattle. They stir and seem apprehensive at the sound of a raucous rattle. Two-month-old infants will hold light, small rattles for a short period of time but then drop them. They are attuned to mobiles or cradle gyms strung across their crib. They continue to spend a great deal of time just watching the people around them.
- 3-month-old: Three-month-old infants can handle small blocks or small rattles.
- 4-month-old: Four-month-olds need a playpen or a sheet spread on the floor so they have an opportunity to exercise their new skill of rolling over. Rolling over may be so intriguing that it can serve as a toy for the entire month.
- 5-month-old: Five-month-old infants are ready for a variety of objects to handle, such as plastic rings, blocks, squeeze toys, clothespins, rattles, and plastic keys. Check that all of these are small enough that an infant can lift them with one hand, yet big enough that he or she cannot possibly swallow them.
- 6-month-old: A 6-month-old child can sit steadily enough to be ready for bathtub toys such as rubber ducks or plastic boats if carefully supervised. Because they are starting to teethe, most at this age enjoy a teething ring to chew on.
- 7-month-old: Because 7-month-old infants can transfer toys, they are interested in items such as blocks, rattles, or plastic keys that are small enough to be transferred easily. As their mobility increases, they begin to be more interested in brightly colored balls or toys that previously rolled out of reach.
- 8-month-old: Eight-month-old infants are sensitive to differences in texture. They enjoy having toys with different feels to them, such as velvet, fur, and fuzzy, smooth, or rough items.
- 9-month-old: The 9-month-old infant needs the experience of creeping. This means time out of a crib or playpen so there is room to maneuver. Many 9-month-olds begin to enjoy toys that go inside one another, such as a nest of blocks or rings of assorted sizes that fit on a center post. Some are more interested in pots and pans that stack rather than toys.
- 10-month-old: By 10 months, infants are ready for peek-a-boo and will spend a long time playing the game with their hands or with a cloth over their head that they can easily reach and remove. They can clap, so they are also ready to play patty-cake.
- 11-month-old: By 11 months, children have learned to cruise or walk by holding on to low tables. They often find this so absorbing that they spend little time doing anything else during the month.
- 12-month-old: Twelve-month-old infants enjoy putting things in and taking things out of containers. They like little boxes that fit inside one another or dropping small blocks into a larger box. As soon as they can walk, they will be interested in pull toys. A lot of time may be spent listening to someone saying nursery rhymes or listening to music.
Development of Senses
- Vision:
- One-month-old infants are able to regard an object in the midline of their vision (something directly in front of themselves) as soon as it is brought in as close as about 18 in. (46 cm). They follow the object a short distance if it moves but not across the midline as yet. They study or regard a human face with a fixed stare.
- Two-month-old infants focus well (from about age 6 weeks) and so are able to follow moving objects with the eyes (although still not past the midline). This indicates a major development—binocular vision.
- Three-month-old infants can follow an object across their midline. They typically hold their hands in front of their face and study their fingers for long periods of time (hand regard).
- Four-month-old infants are able to recognize familiar objects, such as a frequently seen bottle, rattle, or toy animal. They eagerly follow their parents’ movements with their eyes.
- By 6 months, infants are capable of organized depth perception. This increases the accuracy of their reach for objects as they begin to perceive distances correctly.
- Seven-month-olds pat their own image in a mirror. Their depth perception has matured to the extent that they can perform such tasks as transferring toys from hand to hand.
- By 10 months, an infant looks under a towel or around a corner for a concealed object (the beginning of object permanence, or an awareness that an object out of sight still exists).
- Hearing: That an infant can hear can be demonstrated at birth by the way a newborn quiets momentarily at a distinctive sound such as a bell or a squeaky rubber toy. By 1 month, this reaction is even more marked.
- Hearing awareness becomes so acute by 2 months of age that infants will stop an activity at the sound of spoken words.
- Many 3-month-old infants turn their head to attempt to locate a sound.
- At 4 months of age, when infants hear a distinctive sound, they turn and look in that direction.
- By 5 months of age, infants demonstrate they can localize sounds downward and to the side, by turning their head and looking down.
- Six-month-olds have progressed to being able to locate sounds made above them.
- By 10 months, infants can recognize their name and listen acutely when spoken to.
- By 12 months, infants can easily locate sounds in any direction and turn toward them. A vocabulary of two words plus “ma-ma” and “da-da” also demonstrates that an infant can hear.
- Touch: Infants need to be touched so they can experience skin-to-skin contact. Clothes should feel comfortable and soft rather than rough; diapers should be dry rather than wet. Teach parents to handle infants with assurance yet gentleness.
- Taste: Infants demonstrate they have an acute sense of taste by turning away from or spitting out a taste they do not enjoy. When infants are introduced to solid food at about 6 months, urge parents to make mealtime a time for fostering trust as well as supplying nutrition by being certain feedings are done at an infant’s pace and the amount offered fits the child’s needs and not the parent’s idea of how much should be eaten.
- Smell: Infants can smell accurately within 1 or 2 hours after birth. They respond to an irritating smell by turning their head away from it. They appear to enjoy pleasant odors and learn early in life to identify the familiar smell of breast milk.
Emotional Development
Socialization, or learning how to interact with others, is an extensive phenomenon.
- One month-old infants show they can differentiate between faces and other objects by studying a face or the picture of a face longer than other objects. They are calm and feed well for the person who has been their primary caregiver.
- 1 ½-month-old: When an interested person nods and smiles at a 6-week-old infant, the infant smiles in return. This is a social smile and is a definite response to the interaction, not the faint, quick smile that younger infants, even newborns, demonstrate. It is a major milestone because it reflects growing maturity in a number of areas, most notably vision, motor control, and intelligence.
- By 3 months, infants demonstrate increased social awareness by readily smiling at the sight of a parent’s face. Three-month-old infants laugh out loud at the sight of a funny face.
- By 4 months, when a person who has been playing with and entertaining an infant leaves, the infant is likely to cry or show that the interaction was enjoyable. Infants at this age recognize their primary caregiver and prefer that person’s presence to others.
- By 5 months, infants may show displeasure when an object is taken away from them. This is a step beyond showing displeasure when a person leaves.
- By 6 months, infants are increasingly aware of the difference between people who regularly care for them and strangers. They may begin to draw back from unfamiliar people.
- Seven-month-old infants begin to show obvious fear of strangers. They may cry when taken from their parent, attempt to cling to the parent, and reach out to be taken back.
- During the eighth month, the infant’s fear of strangers reaches its height, so much so that this phenomenon is often termed eighth-month anxiety, or stranger anxiety (Levine, 2011). Remember that an infant at the height of this phase will not go willingly from a parent’s arms to a nurse’s arms. Taking a few minutes to talk to the child and parent first so you are perceived as a friend, not a stranger, is time well spent.
- Nine-month-old infants are very aware of changes in tone of voice. They cry when scolded not because they understand what is being said but because they sense their parent’s displeasure.
- By 12 months, most children have overcome their fear of strangers and are alert and responsive again when approached. They like to play interactive nursery rhymes and rhythm games and “dance” with others. They also like being at the table for meals and joining in family activities.
Cognitive Development
In the first month of life, an infant mainly uses simple reflex activity. There is little evidence infants at this early age see themselves as separate from their environment. However, this does not mean they cannot respond actively or interact with people. They demonstrate they are very people oriented moments after birth by cuddling against an adult’s chest.
- Primary Circular Reaction: in the third month of life, a child enters a cognitive stage identified by Piaget as primary circular reaction. During this time, the infant explores objects by grasping them with the hands or by mouthing them. Infants appear to be unaware of what actions they can cause or what actions occur independently, however. For example, an infant’s hand may strike the mobile, causing it to move an entertain the infant, but this does not prompt the infant to strike the mobile again, as they do not realize their hand caused the movement.
- Secondary Circular Reaction: in the sixth month of life, infants pass into a stage Piaget as secondary circular reaction. The infant begins to realize how they affect the environment. In the earlier example, they instead realize now that their hand caused the mobile to move, and so they repeat their action and hit it again.
- Object Permanence: By 10 months, infants discover object permanence. Infants are ready for peek-a-boo once they have gained this concept. They know their parent still exists even when hiding behind a hand or blanket and wait excitedly for the parent to reappear.
- As infants reach 1 year of age, they are capable of reproducing new events (they deliberately hit a mobile once, it moves, and they hit it again). They drop objects from a high chair or playpen and watch where they fall or roll. This is a frustrating activity for parents because it involves a great deal of reaching and picking up. It is an important activity for infants, however because it confirms their awareness of the permanence of objects and how they are able to control events in their world.
Summary of Infant Growth and Developmental Milestones
| Month | Motor Development | Fine Motor Development | Socialization and Language | Time Reflexes Fade | Play |
|---|---|---|---|---|---|
| 0–1 | Largely reflex actions | Keeps hands fisted; able to follow object to midline with eyes | Enjoys watching face of primary caregiver; needs play time in prone position | ||
| 2 | Holds head up when prone | Demonstrates social smile | Makes cooing sounds; differentiates cry | Grasp reflex fading | Enjoys bright colored mobiles |
| 3 | Holds head and chest up when prone | Follows object past midline with eyes | Laughs out loud | Landau reflex is strong | Spends time looking at hands (hand regard); “tummy time” important during the day |
| 4 | Turns back to front; no longer has head lag; bears partial weight on feet | Stepping, tonic neck, extrusion reflexes are fading | Needs space to practice turning | ||
| 5 | Should turn readily front to back and back to front | Tonic neck reflex fading | Handles rattles well | ||
| 6 | Beginning to show ability to sit | Uses palmar grasp | May say vowel sounds (oh oh) | Moro and tonic neck reflex have faded | Enjoys bathtub toys, rubber ring for teething |
| 7 | Reaches out to be picked up; first tooth (central incisor) erupts | Transfers objects hand-to-hand | Shows beginning fear of strangers | Likes objects that are good size for transferring | |
| 8 | Sits securely without support | Fear of strangers peaks | Enjoys manipulation, rattles, and toys of different textures | ||
| 9 | Creeps or crawls (abdomen off floor) | Says first word (da-da) | Needs safe space for creeping | ||
| 10 | Pulls self to standing | Uses pincer grasp (thumb and finger) to pick up small objects | Plays games like patty cake and peek-a-boo | ||
| 11 | Cruises (walks with support) | Cruising can be main activity | |||
| 12 | Stands alone; some infants take first step | Holds cup and spoon well; helps to dress (pushes arm into sleeve) | Says two words plus ma-ma and da-da | Landau reflex fades | Likes toys that fit inside each other (pots and pans); nursery rhymes; will like pull toys as soon as walking |
Nursing Roles in Health Promotion During Infancy
The infant’s developmental task, as proposed by Erikson, is to form a sense of trust. Infants with numerous caregivers, inconsistent feeding and care, or who don’t always have their needs met can have difficulty learning to trust. It is important for infants to establish the ability to love, or trust, early in life in this way because development is sequential. If a first developmental step is inadequate, this inadequacy can pervade all future steps. In reference to trust, the end result could be an adult unable to instill a sense of trust in his or her own child, perpetuating the inadequacy from generation to generation.
To encourage a sense of trust in an infant requires a sense of confidence that one can predict what is coming next. This does not equate to a rigid schedule of care—it does imply that parents should study their infant’s reactions to activities and then establish a workable schedule based on that (e.g., breakfast, bath, playtime, nap, lunch, walk outside, quiet playtime, dinner, story, and bedtime). This gentle rhythm of care gives infants a sense of being able to predict what is going to happen and gives life consistency. Routine is important. This involves who is providing care. It is important that care is mainly given by one person.
| Area of Care in an Ill Infant | Nursing Actions |
|---|---|
| Nutrition |
|
| Dressing Changes |
|
| Medication Administration |
|
| Rest |
|
| Hygiene |
|
| Pain |
|
| Stimulation |
|
Promoting Infant Safety
- Aspiration: Infants are prolific mouthers. They will bring objects they can grasp to their mouth to interact with it. Make sure these objects are either safe to eat or too big to fit in the mouth. Food such as popcorn or peanuts are easily aspirated. Inspect toys and pacifiers for small, detachable parts that could be aspirated.
- Small, cylindrical objects are more dangerous than square or flexible objects. These are able to lodge into the airway and cause complete obstruction.
- Decorative items on clothing can also be aspirated, such as buttons. Detachable or easily broken components are, in general, a common source of aspirated objects. These include toys, rattles, and even pacifiers.
- When solid foods are introduced, encourage parents to offer small pieces of hot dogs or grapes, not large chunks for this reason. Children under about 5 years of age should not be offered popcorn or peanuts because of the danger of aspiration.
- Falls: never leave an infant on an unprotected surface, such as a bed or couch, even if the infant is in an infant seat. Gates should be placed at the top and bottom of stairways. If the infant is able to locomote, they should not do so while holding a sharp object or any object that could cause injury when falls occur. Crib rails should be securely raised and locked. Supervision is required during the use of a high chair. Walkers should not be used near stairways.
- Teach parents to be prepared for their infant to turn over by 2 months of age. From that time on, they must be especially vigilant not to leave the baby unattended on a changing table or counter.
- Motor Vehicle: a well-tethered age-appropriate back-facing seat in the back seat of the car is a requisite for transporting an infant in an automobile. Do not be distracted by an infant while driving. Do not leave an infant unattended in a parked car.
- Suffocation: do not leave plastic bags within the infant’s reach. Pillows are not kept in the crib. Unused appliances should have doors removed to prevent trapping. Cribs should be approved for safety. Constricting clothing (e.g., bib, pacifier string) should be removed from neck at bedtime.
- Drowning: Do not leave infants along in a bathtub or unsupervised near water, even buckets of cleaning water.
- Animal Bites: do not allow an infant to approach a strange dog; supervise with family pets.
- Poisoning: Never present medication as candy; buy medications in containers with safety caps; put away in a high cabinet immediately after use; never leave medication in a pocket or handbag. Never take medication in front of infants. Lead-based paint should not be used in any area of the home. Plants should be hung or set on high surfaces.
- Burns: Test warmth of formula and food before feeding, especially if warmed by a microwave. Do not smoke or drink hot liquids while holding or caring for an infant. Handles of pans should be turned toward the back of the stove.
- Use a sunscreen on a child over 6 months when out in direct or indirect sunlight and limit the child’s sun exposure to less than 30 minutes at a time.
Promoting Nutritional Health in Infants
- Breast Milk: the best food during the first 12 months of life (and the only food necessary for the first 6 months) is breast milk. Exclusive breastfeeding for 6 months is recommended, then optimally breastfeeding continues through the entire first year.
- A breastfed or partially breastfed infant should receive 400 IU of vitamin D supplement starting at 2 weeks of age.
- For infants whose mothers choose not to or are unable to breastfeed, a commercial iron-fortified formula will supply adequate nutrition for the infant year. Although after 6 months, if the water supply does not contain fluoride, fluoride may need to be supplemented. Infants who are changed to cow’s milk before 1 year of age should receive a supplementary form of vitamin C and iron and possibly fluoride to make up for the deficiency of these components in cow’s milk. However, the practice of switching to cow’s milk is not recommended because the protein in it is difficult for an infant to digest, possibly leading to such intestinal irritation that slight but continuous gastrointestinal bleeding occurs, which results in anemia.
- Dietary Allowances: The entire first year of life is one of extremely rapid growth, so a high-protein, high calorie intake is necessary. Calorie allowances can be gradually reduced during the first year from a level of 120 calories per kilogram of body weight (50 to 55 calories per pound) at birth to approximately 100 calories per kilogram (45 calories per pound) of body weight at the end of the first year to prevent babies from becoming overweight.
- Introduction of Solid Food: A normal full-term infant can thrive on breast milk or a commercial iron-fortified formula without the addition of any solid food until 6 month. Delaying the introduction of solid foods can help reduce kidney load, susceptibility to obesity, and development of food allergies.
- Generally speaking, parents can tell infants are physiologically ready for solid food when they are nursing vigorously every 3 to 4 hours and do not seem satisfied or when they are taking more than 32 oz (960 ml) of formula a day and do not seem satisfied.
- Infants are not ready to digest complex starches until amylase is present in saliva at approximately 2 to 3 months. Biting movements begin at approximately 3 months. Chewing movements do not begin until 7 to 9 months. Therefore, foods that require chewing should not be given until this age.
- In addition to these cautions, the extrusion reflex needs to fade before infants accept food readily. With the extrusion reflex intact, when anything is placed on the anterior third of an infant’s tongue, it is automatically extruded or thrust out of the mouth by the tongue. This is a lifesaving reflex in early infancy because it prevents infants from swallowing or aspirating foreign objects that touch the mouth. The reflex fades at 3 to 4 months at about the same time the gastrointestinal tract has matured to be ready to digest solid food.
- A newborn’s stomach can hold approximately 2 tablespoons (30 ml). By 1 year, a stomach can hold no more than about 1 cup (240 ml). For this reason, when they begin eating solid food, infants rarely take more than 2 tablespoons (30 ml) at a time.
Feeding Pattern
A typical pattern for the introduction of solid food beginning at 6 months includes:
- Iron-fortified infant cereal mixed with breast milk, orange juice, or formula; it aids in preventing iron-deficiency anemia, is the least allergenic type of food, and is the most easily digested so it is usually the first food offered.
- Vegetables; these are a good source of vitamin A and add new texture and flavors to the diet.
- Fruit; these are the best sources of vitamin C and a good source of vitamin A.
- Meat is a good source of protein, iron, and B vitamins. It is usually introduced at 9 months of age because this is the time an infant’s iron stores are beginning to be depleted.
- By 6 months of age, egg yolk, a good source of iron, can be added. Egg whites, common allergens, are not included.
Teach parents to offer new foods one at a time and to allow their child to eat that item for about 3 to 7 days before introducing another new food. This system helps parents to detect a possible food allergy in addition to allowing the infant to get used to the new experience.
Foods to Avoid
Caution parents to omit wheat, tomatoes, oranges, fish, and egg whites if there are allergies in the family because these foods are those most likely to cause allergies. Also, parents should never use honey as a sweetener because it may contain botulism spores and never use cow’s milk because it can cause microscopic intestinal bleeding.
If a parent is going to prepare baby food, the parent needs to avoid preparing spinach, carrots, beets, green beans, and squash because these can contain excessive amounts of nitrates that are not processed well by infants. Commercial baby food has the nitrates removed and so does not present this problem.
- Weaning: after the advised first 6 months of exclusive breastfeeding, infants continue to eat with complementary solids for the first full year. Infants can drink effectively from a cup at about 9 months of age, coinciding with the diminishing sucking reflex from the 6th to 9th month. At this point, weaning from bottles should be considered by parents.
- To wean from either formula or breastmilk, the parent chooses one feeding a day and begin offering fluid by the new method at that feeding. The time of day is not important, besides avoiding times when the infant is usually fussy. There is no prescribed duration to how long it will take to complete weaning.
- Self-Feeding: at approximately 6 months of age, infants become interested in handling a spoon and beginning to feed themselves (with a great deal of spilling). Self-feeding at this point is more efficient with their fingers. Allowing a child to self-feed is good practice, albeit messy. The parent can quietly help the fatigued or frustrated infant without making an issue of it. Once infants begin to play with food, e.g., squeezing it through their fingers, or dabbing it in their hair, it is time to end the meal. Infants who are hungry eat; those who are full, play.
A Vegetarian Diet
An infant eating a vegetarian diet should continue to be breastfed or ingest an iron-fortified commercial formula for the entire first year. As with all infants, an assortment of foods should be provided, including vegetables such as peas, potatoes, and carrots; fruits such as apples, prunes (which are high in iron), and bananas; infant cereal; tofu; wheat germ; legumes; brewer’s yeast; and synthetic vitamin D.
Promoting Infant Development in Daily Activities
- Bathing: a daily bath is not necessary except in very hot weather. Washing can be limited to the infant’s face, hands, and diaper area washed. Bath time should be enjoyable for an infant and can serve many functions other than just the obvious one of cleanliness. Opportunity for play, learning different textures and sensations, exercise, and child-parent bonding are all present during bath time. Teach parents to never leave infants along in a tub even if they are supported by an infant seat because they could easily slip under the water and drown.
- Diaper-Area Care: good diaper-area hygiene is to change diapers frequently, about every 2 to 4 hours. However, it is rarely good practice to interrupt the child’s sleep to change diapers. If rashes develop from sleeping in wet diapers, air drying or sleeping without a diaper may be a solution.
- At each diaper change, parents should wash the skin with clear water or a commercial alcohol-free diaper wipe and then pat or allow the skin to air dry.
- Parents should not use baby powder, as it is a potential source of aspiration.
- Dental Care: exposing teeth to fluoride is one of the most effective ways to promote health tooth formation and prevent tooth decay. A water level of 0.3 ppm fluoride in water is recommended because this is the level that protects tooth enamel best yet does not lead to staining of teeth. If fluoride supplementation is inadequate, fluoride drops or fluoride toothpaste is recommended beginning at 6 months of age.
- Toothbrushing can begin even before teeth erupt by rubbing a sot washcloth over the gum pads. This eliminates plaque and reduces the presence of bacteria, creating a clean environment or the arrival of first teeth. Once teeth erupt, all surfaces should be brushed with a soft brush or washcloth once or twice a day.
- An initial dental checkup should be made before 2 years of age, and checkups should continue at 6-month intervals until adulthood.
- Sleep: sleep needs and habits vary greatly among infants, but most require 10 to 12 hours of sleep at night and one or several naps during the day. Parents are advised to separate the infant’s sleeping space somewhere close by but not in their bed. This allows parents to gain better sleep, and teach the infant to quiet themselves an go back to sleep should they awaken briefly.
Sudden Infant Death Syndrome
Do not place pillows in an infant’s crib. Always place an infant on his or her back to sleep because this position markedly reduces the incidence of sudden infant death syndrome (SIDS). In addition to supine positioning, use of a firm sleep surface, breastfeeding, room sharing without bed sharing, routine immunizations, considering the use of a pacifier, and avoidance of overheating, closed spaces, and exposure to tobacco smoke are other suggestions for helping to prevent the syndrome.
- Exercise: infants benefit from outings in a carriage or stroller because sunlight provides a natural source of vitamin D. In hot weather, caution parents to protect an infant from sunburn by exposing the child to the sun for only very short periods, beginning with 3 to 5 minutes the first day, a little more the next day, and so on up to 15 to 20 minutes at a time. The sun is most intense between 10 a.m. and 3 p.m., so early mornings and late afternoons are the best times for infants to be outside.
Nursing Care of a Family with a Toddler
During the toddler period, the age span from 1 to 3 years, children accomplish a wide array of developmental tasks and change from largely immobile and preverbal infants who are dependent on caregivers for the fulfillment of most needs to walking, talking young children with a growing sense of autonomy (independence). To match this growth, parents must also change during this period.
Physical Growth
Compared to infancy, growth slows down during toddlerhood. Great strides are found instead in development.
- Weight, Height, Head Circumference, and Body Mass Index:
- A child gains only about 5 to 6 lb (2.5 kg) and 5 in. (12 cm) a year during the toddler period, much less than the rate of growth during the infant year.
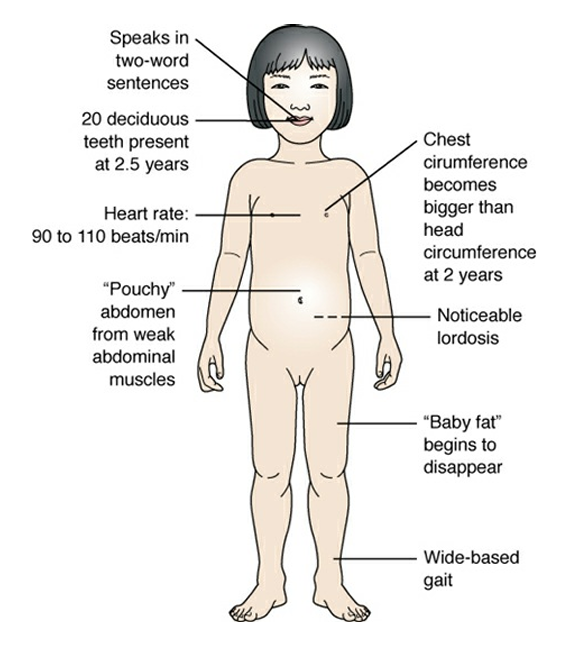
- Head circumference increases only about 2 cm during the second year compared to about 12 cm during the first year. Head circumference equals chest circumference at 6 months to 1 year of age. By 2 years, chest circumference should have grown greater than that of the head.
- Body Contour: the infant appears lordotic with a protuberant abdomen due to weak abdominal muscles. As they become more experienced at walking, this will correct itself naturally.
- Body Systems:
- Respirations slow slightly but continue to be mainly abdominal.
- Control of the urinary and anal sphincters becomes possible with complete myelination of the spinal cord so toilet training is possible.
- Immune globulin (Ig)G and IgM antibody production becomes mature at 2 years of age. The passive immunity obtained during intrauterine life is no longer operative.
- In the respiratory system, the lumens of vessels enlarge progressively so the threat of lower respiratory infection lessens.
- Stomach secretions become more acid; therefore, gastrointestinal infections also become less common.
- Teeth: Eight new teeth (the canines and the first molars) erupt during the second year. All 20 deciduous teeth are generally present by 2.5 to 3 years of age (Bishop, 2011).
Language Development
Toddlerhood is a critical time for language development, although even this varies among children because to master language, children need practice time. A child who is 2 years old and does not talk in two-word, noun–verb simple sentences needs a careful assessment to determine the cause because this implies underdevelopment.
- A word that is used frequently by toddlers and that is a manifestation of their developing autonomy is “no.” Toddlers may use the word to mean they are refusing a task, that they do not understand it, or they may only be practicing a sound they have noticed has potent effects on those around them.
- Urge parents to encourage language development by naming objects (e.g., ball, block, music box, doll) as they play with their child or when they give the toddler something (“Here is your drink of water,” “Let’s put on these pajamas,” etc.).
- Because children learn language from imitating what they hear, if they are spoken to in baby talk, their enunciation of words can be poor; if they hear examples of bad grammar, they will not use good grammar.
Emotional Development
Children change a great deal in their ability to understand the world and how they relate to people during the toddler years.
- Autonomy: according to Erikson, the toddler years herald the developmental task of the development of a sense of autonomy versus shame or doubt. Children who have learned to trust themselves and others during the infant year are better prepared to do this than those who have not learned to trust themselves or others. To develop a sense of autonomy is to develop a sense of independence. A healthy level of autonomy is achieved when parents are able to balance independence with consistently sound rules for safety.
- Socialization: Once toddlers are walking well, they become resistant to sitting in laps and being cuddled. This is not lack of a desire for socialization but a function of being independent.
- At 15 months, children are still enthusiastic about interacting with people, providing those people are willing to follow them where they want to go.
- By 18 months, toddlers imitate the things they see a parent doing, such as “study” or “sweep,” so they seek out parents to observe and imitate.
- By 2 or more years of age, children become aware of gender differences and may point to other children and identify them as “boy” or “girl.”
- Play: All during the toddler period, children play beside other children, not with them. This side-by-side play (parallel play) is not unfriendly but is a normal developmental sequence that occurs during the toddler period. Caution parents that if two toddlers are going to play together, they must provide similar toys because an argument over one toy is likely to occur.
- The toys toddlers enjoy most are those they can play with by themselves and that require action (e.g., push-pull toys). Trucks they can make go, squeaky frogs they can squeeze, rocking horses they can ride, pegs they can pound, and a toy telephone they can talk into are all favorites. These are all toys children can control, giving them a sense of power in manipulation, which is an expression of autonomy.
- At 15 months of age, children are still in a put-in, take-out stage, so they continue to enjoy stacks of boxes that fit inside each other. They enjoy throwing toys out of a playpen or from a high chair tray as long as someone will pick them up and return them again and again.
- The 18-month-old child walks securely enough to enjoy pull toys. Toys should be strong enough to take a great deal of abuse because children this age may use toys in ways other than those for which they were designed. There is no need for parents to correct children about the way they are using a toy as long as it is safe and appears to give satisfaction.
- By age 2 years, when toddlers begin to spend time imitating adult actions in their play such as wrapping a doll and putting it to bed or “driving the car,” they begin to use fewer toys than before. The act of imitating has become their play. By the end of the toddler period, both boys and girls begin to like roughhousing and spend at least part of every day in this very active, stimulating type of play.
Cognitive Development
As a toddler, a child enters the final stages of Piaget’s sensorimotor thought and the beginning of the preoperative period at approximately 12 months. During the fifth and sixth stages of the sensorimotor phase, toddlers are described as “little scientists” because of their interest in trying to discover new ways to handle objects or new results that different actions can achieve. By stage 6 of cognitive development (between 18 and 24 months of age), toddlers are able to try out various actions mentally rather than having to actually perform them—the beginning of problem solving or symbolic thought.
- Children at this stage have a type of faulty reasoning (prelogical reasoning) that can lead them to wrong conclusions and faulty judgment. Daddy is shaving; therefore, he must be going to work because he went to work after he shaved yesterday.
- Children at this stage are also able to remember an action and imitate it later (deferred imitation); they can do such things as pretend to drive a car or put a baby to sleep because they have seen this previously and not just in the recent past. Object permanence becomes complete.
Nursing Roles in Health Promotion During Toddlerhood
Promoting Toddler Safety
Accidents (unintentional injuries) are the major cause of death in infants through late adolescents in the United States. Unintentional ingestions (poisoning) and auto accidents are the types of unintentional injuries that occur most frequently in toddlers.
- General: Know whereabouts of toddlers at all times. Toddlers can climb onto chairs or high stools they could not manage before, can turn door knobs and go places they could not go before, and are able to pull a television set over on top of themselves
- Motor Vehicles: Maintain your child in a car seat; do not be distracted by the child from safe driving. Do not allow the child to play outside unsupervised. Supervise toddlers with pedaling toys (e.g., look before crossing driveways, do not cross streets) but do not expect toddler will obey these rules at all times (i.e., stay close by).
- Falls: Gates should be placed at the top and bottom of stairways. If the infant is able to locomote, they should not do so while holding a sharp object or any object that could cause injury when falls occur. Crib rails should be securely raised and locked.
- Aspiration: Do not feed toddler popcorn or nuts; caution child not to eat while running. Do not leave toddler alone with a balloon. Examine toys for small parts that could be aspirated; remove toys that appear dangerous.
- Drowning: Do not leave toddler alone in a bathtub or near water (including buckets of cleaning water). Fence pools; insist toddlers wear safety “floats” or life vests; supervise at all times when near water.
- Animal Bites: Do not allow toddler to approach strange dogs. Supervise child’s play with family pets.
- Poisoning: Never present medication as candy or take medication in front of child, purchase containers with childproof caps, store them securely in locked cabinets or cabinets out of reach of the child. Batteries, magnets, and other poisonous ingestible substances should be stored safely.
- Burns: Cook on the back burners of stove if possible; turn handles of pots toward back of stove to prevent toddler from reaching up and pulling them down. Keep screen in front of fireplace or heater. Do not allow toddlers to blow out matches (teach fire is not fun); store matches out of reach.
Promoting Nutritional Health in Toddlers
Because growth slows abruptly after the first year of life, a toddler’s appetite is usually less than an infant’s. Children who ate hungrily 2 months earlier now may sit and play with their food. Because the actual amount of food eaten daily varies from one child to another, teach parents to place a small amount of food on a plate and allow their child to eat it and ask for more rather than serve a large portion that the child cannot finish. Allowing self-feeding is a major way to both strengthen independence in a toddler and improve the amount of food consumed. Offering finger foods such as pieces of chicken, slices of banana, pieces of cheese, and crackers and allowing a choice between two types of food helps promote independence while exposing children to varied foods.
- Dietary Allowances:
- Sedentary children ages 1 to 3 years should consume 1,000 kcal daily; active children in this age group may need up to 1,400 kcal daily
- Calories are best supplied by a variety of foods spaced into three meals a day.
- Protein and carbohydrate needs are often those most easily met during the toddler period; diets high in sugar should be avoided to help prevent toddler obesity.
- Fats should generally not be restricted for children under 2 years old; however, children over 2 years old should have a total fat intake between 30% and 35% of calories, with most fat coming from sources of polyunsaturated and monounsaturated fatty acids, such as fish, nuts, and vegetable oils, the same as adults.
- Trans fats should be kept to a minimum.
- Adequate calcium and phosphorus intake is important for bone mineralization. Milk should be whole milk until age 2 years, after which 2% milk can be introduced.
A Vegetarian Diet
Vegetarian diets are adequate for toddlers if parents are well informed about needed vitamins and minerals. A vegetarian diet can be easily designed for a toddler who prefers finger foods because many vegetables, fruits, and grains such as pieces of oranges, peaches, raisins, chickpeas, and crackers are easily eaten this way. The use of fortified soy milk prevents fluid, protein, vitamin B12, and calcium deficiencies. Tofu should be served often to supply protein.
Promoting Toddler Development in Daily Activities
- Dressing: By the end of the toddler period, most children can put on their own socks and underpants. Some may also be able to pull on slacks, pullover shirts (the sleeves of a shirt often confuse a toddler), or simple dresses.
- Sleep: The amount of sleep children need gradually decreases as they grow older. They may begin the toddler period napping twice a day and sleeping 12 hours each night and end it with one nap a day and only 8 hours of sleep at night. If a child has difficulty falling asleep at night, it may be time to omit or shorten an afternoon nap. If a child is so short tempered at dinnertime that eating is impossible, perhaps the child needs two naps a day.
- As with any other activity of this period, a toddler loves a bedtime routine: bath, pajamas, a story, toothbrushing, being tucked into bed, having a drink of water, choosing a toy to sleep with, and turning out the lights.
- Many toddlers are ready to be moved out of a crib into a youth bed or regular bed with protective side rails or a chair strategically placed beside it by the end of the toddler period. Remind parents to stress that sleeping in a regular bed does not give children the right to get in and out of bed as they choose. When first moved to a bed without side rails, many children are found sleeping on the floor of the room in the morning. There is no harm in this unless it is cold or drafty.
- Dental Care: Toddlers often need between-meal snacks. To help prevent dental caries from frequent snacking, encourage parents to offer fruit (e.g., bananas, pieces of apple, orange slices) or protein foods (e.g., cheese, pieces of chicken) for snacks rather than high carbohydrate items such as cookies to limit exposure of the child’s teeth to carbohydrate. Calcium (found in large amounts in milk, cheese, and yogurt) is especially important for the development of strong teeth and so are other good snack foods. In addition, children should continue to drink fluoridated water or, if not available, receive fluoride supplements so all new teeth form with cavity-resistant enamel.
- Remind parents not to put a child to bed with a bottle of milk or juice to help prevent the development of caries. Toddlers need a toothbrush they recognize as their own. Toward the end of the toddler period, they can begin to do the brushing themselves under supervision (almost all children need some supervision until about age 8 years).
Parental Concerns Associated with the Toddler Period
- Toilet Training is one of the biggest tasks a toddler tries to achieve. It may also be perceived as an expression of autonomy. It is an individualized task for each child, beginning and finishing according to a child’s ability to accomplish it, not according to a set schedule.
- Before children can begin toilet training, they must have reached three important developmental levels, one physiologic and the other two cognitive:
- They must have control of rectal and urethral sphincters, usually achieved by the time they walk well. This may not be achieved until at least the end of the first year, when tracts of the spinal cord are myelinated to the anal level (coinciding with a child’s ability to walk well).
- They must have a cognitive understanding of what it means to hold urine and stools until they can release them at a certain place and time. Cognitively and socially, many children do not understand what is being asked of them until they are 2 or even 3 years old.
- They must have a desire to delay immediate gratification for a more socially accepted action.
- The markers of readiness are subtle, but as a rule, children are ready for toilet training when they begin to be uncomfortable in wet diapers. They demonstrate this by pulling or tugging at soiled diapers, or they may bring a parent a clean diaper after they have soiled so they can be changed.
- Defecation training is much easier to grasp than urination. Routine times can also be expected of bowel movements. Sit the child on the potty chair or toilet at the time they usually defecate. Praise the child if they do defecate, and remind them to wash their hands afterward.
- Some toddlers have difficulty remaining dry at night until they are 3 to 4 years old. Do not pressure your child to accomplish nighttime dryness but assume he is doing the best he can.
- Before children can begin toilet training, they must have reached three important developmental levels, one physiologic and the other two cognitive:
- Ritualistic Behavior: Although toddlers spend a great deal of time every day investigating new ways to do things and trying activities they have never done before, they also enjoy ritualistic patterns. They will use only “their” spoon at mealtime or only “their” blanket at bedtime.
- Negativism: As part of establishing their identities as separate individuals, toddlers typically go through a period of extreme negativism. They do not want to do anything a parent wants them to do. Their reply to every request is a very definite “no.” This change indicates toddlers have learned that they are separate individuals with separate needs. It is important toddlers do this if they are to grow up to be persons who are independent and able to take care of their own needs and desires.
- Once it runs its course, extreme negativism will pass. In the meantime, the more parents try to make children obey them, the more children are likely to resist. Some long-term parent–child interaction problems begin during this period because parents insist on being obeyed totally or are inconsistent in their approach.
- A toddler’s “no” can best be reduced by limiting the number of questions asked of the child. Conversion of questions, e.g. “Are you ready for dinner?”, into statements, e.g. “Come to the table. It’s dinnertime.”, can help avoid many negative responses. However, toddlers still benefit from decision making. To allow such opportunities, secondary choices such as “It’s dinnertime. Do you want to use a big or little plate?” allow children to exercise autonomy.
- Discipline: Remind parents that discipline and punishment are not interchangeable terms. Discipline means setting rules or road signs so children know what is expected of them. Punishment is a consequence that results from a breakdown in discipline or the child’s disregard of the rules that were learned.
- Generally, (a) parental discipline should be consistent, and (b) rules are learned best if correct behavior is praised rather than wrong behavior punished.
- Separation Anxiety: fear of being separated from parents begins at about 6 months of age and persists throughout the preschool period. Toddlers who have separation anxiety have difficulty accepting being separated from their primary caregiver to spend the day at a day care center or if they or their primary caregiver is hospitalized.
- Most toddlers react best to separation if a regular babysitter is employed or if the day care center has consistent caregivers. It helps if toddlers have fair warning they will have a babysitter.
- It helps if parents say goodbye firmly, repeat the explanation they will be there when the child wakes in the morning, and then leave. Prolonged goodbyes only lead to more crying. Sneaking out prevents crying and may ease the parents’ guilt, but it can strengthen a child’s fear of abandonment and so should be discouraged. This applies to leaving after hospital visits as well.
- Temper Tantrums: Almost every toddler has a temper tantrum at one time or another. The child may kick; scream; stomp feet; shout, “No, no, no”; flail arms and legs; bite; or bang his or her head against the floor. This occurs because toddlers are independent enough to know what they want, but they do not have the vocabulary or the wisdom to express their feelings in a more socially acceptable way.
- Tantrums may arise from being tired, unrealistic requests by parents (tasks the toddler is unable to perform, “sharing” before the concept is developed in the toddler, or constantly being thwarted by a “no” from the parents). Parents should attempt to determine the reason for the behavior, determine if the behavior is a tantrum and not something else (e.g., seizure activity, neurologic breath holding), and determine the best course of action.
- Probably the best approach is for parents to simply tell a child that they disapprove of the tantrum and then ignore it. They might say, “I’ll be in the bedroom. When you’re done kicking, you come into the bedroom, too.” Children who are left alone in a kitchen this way will usually not continue a tantrum but will stop after 1 or 2 minutes and rejoin their parents. Parents should then accept the child warmly and proceed as if the tantrum had not occurred. This same approach works well for nurses caring for hospitalized toddlers.
Autism Spectrum Disorder
Classic ASD is a complex range of neurodevelopment disorders characterized by communication difficulties, poor social interaction, and frequent repetitive and stereotyped movements. It occurs in all demographics, as frequently as 1 in 88 children, and more frequently in boys than in girls.
Symptoms begin to appear slightly in infancy but are usually obvious enough during the toddler years for parents to become concerned because their child tends not to speak any words, does not make eye contact with others, and has difficulty interacting with playmates, preferring instead to watch a spinning toy, water swirling down the toilet, or repeating sing-song repetitive phrases.
Children need to be screened for autism symptoms by 12 months of age and again at 18 and 24 months of age by observation and parent report.
Summary of Toddler Growth and Development Milestones
| Age (in Months) | Fine Motor | Gross Motor | Language | Play |
|---|---|---|---|---|
| 15 | Puts small pellets into small bottles; scribbles voluntarily with a pencil or crayon; holds a spoon well but may still turn it upside down on the way to mouth | Walks alone well; can seat self in chair; can creep up stairs | 4–6 words | Can stack two blocks; enjoys being read to; drops toys for adult to recover (exploring sense of permanence) |
| 18 | No longer rotates a spoon to bring it to mouth | Can run and jump in place; can walk up and down stairs holding onto a person’s hand or railing; typically places both feet on one step before advancing | 7–20 words; uses jargoning; names one body part | Imitates household chores such as dusting; begins parallel play (playing beside, not with, another child) |
| 24 | Can open doors by turning doorknobs; unscrew lids | Walks up stairs alone, still using both feet on same step at same time | 50 words; two word sentences (noun or pronoun and verb), such as “Daddy go,” “Dog talks” | Parallel play evident |
| 30 | Makes simple lines or strokes for crosses with a pencil | Can jump down from chairs | Verbal language increasing steadily; knows full name; can name one color and holds up fingers to show age | Spends time playing house, imitating parents’ actions; play is “roughhousing” or active |
Nursing Care of a Family with a Preschool Child
The preschool period traditionally includes the years 3, 4, and 5. Although physical growth slows considerably during this period, personality and cognitive growth continue at a rapid rate. Therefore, this is also an important period of growth for parents because they may be unsure how much independence and responsibility for self-care they should allow their rapidly maturing child. Most children of this age want to do things for themselves—choose their own clothing and dress themselves, feed themselves independently, wash their own hair, and so forth.
Each year during the preschool period marks a major step forward in gross motor, fine motor, and language development. Play activities change focus dramatically as the preschooler learns new skills and understands more about the world.
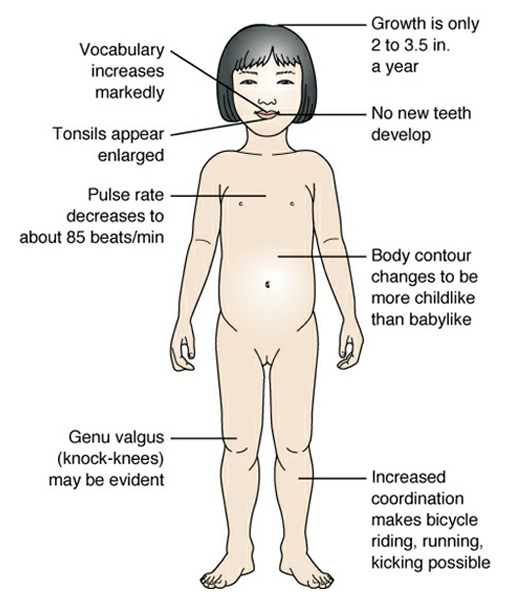
Physical Growth
The wide-legged gait, prominent lordosis, and protuberant abdomen of the toddler change to slimmer, taller, and much more childlike proportions.
- Contour changes are so definite that future body type—ectomorphic body build (slim body build) or endomorphic body build (large body build)—becomes apparent.
- Handedness also begins to be obvious.
- A major step forward is a child’s ability to learn extended language, which is achieved not only by motor development but also by cognitive development.
- Weight gain is slight; the average child gains only about 4.5 lb (2 kg) a year. Appetite remains the same.
- Height gain is also minimal. Only 2 to 3.5 in. (6 to 8 cm) a year on average.
- Head size is no longer routinely measured as it changes little after this period.
- Teeth: children generally have all 20 of their deciduous teeth by 3 years of age; permanent teeth don’t replace these until school age. Preserving these teeth is important because they hold the position for the permanent teeth as the child’s jaw grows larger. If a deciduous tooth has to be removed, children need conscientious follow-up to be certain a space for a permanent tooth remains.
Language Development
The extent of a 3-year-old child’s vocabulary varies depending on how much the child has been encouraged to ask questions or participate in conversations. A child typically, however, has a vocabulary of about 900 words and uses it to ask questions constantly, up to 400 a day, such as “Why is snow cold?” “How do worms hear?” and “What does your tongue do?” A child needs simple answers to such questions to encourage curiosity, vocabulary building, and questioning.
Egocentrism, or perceiving that one’s thoughts and needs are better or more important than those of others, is also strong during the preschool period. Preschoolers cannot believe that not everyone knows facts they know; if asked, “What is your name?” they may reply, “Don’t you know it?” As a part of egocentrism, preschoolers define objects mainly in relation to themselves, so a spoon is “what I eat with,” not a curved metal object; a crayon is “what I write with,” not an orange wax object.
Play
Preschoolers do not need many toys because, with an imagination keener than it will be at any other time in life, they enjoy games that use imitation such as pretending they are a teacher, cowboy or cowgirl, firefighter, or store clerk. Many preschoolers have imaginary friends at this stage (Nielsen, 2012), which often exist until children formally begin school.
Four- and 5-year-olds divide their time between roughhousing and imitative play. Five-year-olds become interested in group games or reciting songs they have learned in kindergarten or preschool.
Emotional Development
Children change a great deal in their ability to understand their world and how they relate to other people during the preschool years.
- Initiative: The developmental task for the preschool-age child is to achieve a sense of initiative versus guilt, as proposed by Erikson. Children with a well-developed sense of initiative like to explore because they have discovered that learning new things is fun.
- If initiative is met with criticism or punishment, a sense of guilt can be developed for wanting to try new activities or to have new experiences. This can carry into school situations after preschool, or even later in life when making decisions about everything from changing jobs to choosing an apartment.
- To gain a sense of initiative, preschoolers need exposure to a wide variety of experiences and play materials so they can learn as much about how things work as possible. They are ready to explore outside their homes such as enjoying a trip to the zoo or an amusement park. They enjoy going with their family on vacation. These types of experiences lead to increased vocabulary.
- Imitation: Imitating the actions of the people around them peaks during preschool age. Role modeling this way should be fun and does not have to be accurate, e.g. a preschooler pretending to be a policeman and putting out fires.
- Fantasy: Toddlers cannot differentiate between fantasy and reality; they believe cartoon characters they see on television are real. Preschoolers, however, begin to make this differentiation. They may become so engrossed in a fantasy role that they fear they are “stuck” in the fantasy and are no longer themselves. Such intense involvement in play is part of “magical thinking,” which is active at this age (i.e., believing thoughts and wishes can come true).
- Oedipus and Electra Complexes: Although the development of Oedipus and Electra complexes may have been overstated by Freud—possibly because of gender bias—many children do seem to manifest such behavior. An Oedipus complex refers to the strong emotional attachment a preschool boy demonstrates toward his mother; an Electra complex is the attachment of a preschool girl to her father.
- Gender Roles: Preschoolers begin to be aware of the difference between sexes and so need to be introduced to both gender roles. Encourage single parents to plan opportunities for their children to spend some time with adults other than themselves, such as a grandparent, a friend, or a relative of the opposite sex, for this experience. If a child is hospitalized during the preschool period, a nurse could readily fill this role.
- Socialization: Because 3-year-olds are capable of sharing, they play with other children their age much more agreeably than do toddlers, which makes the preschool period a sensitive and critical time for socialization (associative play). Preschoolers who are exposed to other playmates have an easier time learning to relate to people than those raised in an environment where they rarely see other children of the same age
- 4-year-olds may argue more as they become more aware of the roles they wish to hold in a group. This is not a regressive change—forward movement involves some testing and identification of their group role.
- 5-year-olds begin to develop “best” friendships. The elementary rule that an odd number of children will have difficulty playing well together generally pertains to children at this age: two or four will play, but three or five will quarrel.
Cognitive Development
According to Piaget (1969), cognitive development is still preoperational by 3 years of age, although children during this period also enter a second phase called intuitional thought. During this second phase of development, children learn by asking questions such as “How come?” and “Why?” Piaget named this stage “intuitive thought” because he believed that children tend to be so certain of their knowledge and understanding that they are unaware of how they gained this knowledge initially.
Intuitive children show a style of thinking he called “centration.” These children typically are focused on the characteristic of an object or person, and they base their decisions or judgment on that one characteristic (as opposed to considering multiple characteristics). For example, a 4-year-old who was asked to put toys into groups might focus his or her attention on the color of the toy instead of the shape or the material from which they are constructed. Centration also means that preschoolers cannot make mental substitutions and often feel they are always right.
Preschoolers are not yet aware of the property of conservation. This means that if they have two balls of clay of equal size, but one is squashed flatter and wider than the other, they will insist the flatter one is bigger (because it is wider) or the intact one is bigger (because it is taller). This inability to appreciate conservation has implications for nursing care because it means preschoolers are not able to comprehend that a procedure performed two separate ways is the same procedure. If the nurse before you, for example, told a child to turn on his right side and then his left side while his bed was made, you may have to allow him to turn those same ways or he will insist you are making his bed wrong. Decentering, combined with the concept of conservation, appear prior to more sophisticated logical thinking abilities.
Moral and Spiritual Development
Children of preschool age determine right from wrong based on their parents’ rules because they have little understanding of the rationale for these rules or even whether the rules are consistent. The rationale “Because my mother says so.” is the answer of a preschooler when asked about why something is right or wrong.
Preschoolers begin to have an elemental concept of spirituality if they have been provided some form of religious training. Belief in an outside force aids in the development of conscience; however, preschoolers tend to do good out of self-interest rather than because of strong spiritual motivation (Kohlberg, 1984).
Nursing Roles in Health Promotion During Preschool Age
Preschoolers are old enough to begin to take responsibility for their own actions. Children’s safety, nutritional health, daily activities, and family functioning are all affected by this increased responsibility.
Promoting Preschooler Safety
As preschoolers broaden their horizons, safety issues must also widen. By age 4 years, children may project an attitude of independence and the ability to take care of their own needs. However, they still need supervision to be certain they do not injure themselves or other children while roughhousing and to ensure they do not stray too far from home.
Imitation can also introduce opportunities for injury, as preschoolers attempt to perform activities outside of their purview such as taking medication they saw their parent taking, handling dangerous objects (e.g., guns, lawn mowers), etc.
A final area to consider is automobile safety. Preschoolers must be reminded repeatedly to buckle their booster seat and not to walk in back of or in front of automobiles. Otherwise, a preschooler’s thought “I want to play with Mary across the street” can be so quick and so intense that the child will run into the middle of the street before remembering street safety rules. Bicycle safety is also important as falls off bicycles are a major cause of severe head injuries in this age group.
Promoting Nutritional Health in Preschoolers
Like the toddler period, the preschool years are not a time of fast growth, so preschool children are not likely to have ravenous appetites. Being certain they get enough daily exercise helps to improve this. A sense of initiative, or learning how to do things, can be strengthened by allowing a child to prepare simple foods, such as making a sandwich or spreading jelly on toast.
Most children are hungry after preschool and enjoy a snack when they arrive home. Because sugary foods can dull a child’s appetite for dinner and it is not too soon to begin measures to prevent childhood obesity, urge parents to offer snacks such as fruit, cheese, or milk rather than cookies and a soft drink or juice.
- Dietary Allowance: As with all age groups, foods selected for preschoolers should include variety (U.S. Department of Agriculture, 2012) and be based on MyPlate (www.choosemyplate.gov) recommendations.
- As long as a child is eating foods from all five food groups and meets the criteria for a healthy child such as being alert and active with height and weight within normal averages, additional vitamins are probably unnecessary.
- If parents do give vitamins, remind them that a child will undoubtedly view a vitamin as candy rather than medicine because of the attractive shapes and colors of preschool vitamins, so they must be stored out of reach. Caution parents not to give more vitamins than the recommended daily amount, or poisoning from high doses of fat-soluble vitamins or iron can result.
A Vegetarian Diet
A vegetarian diet is usually colorful and therefore appeals to preschoolers. Vegetables, fruits, and grains are also healthy snack foods. If vegetarian diets are deficient in any aspects, it is usually in calcium, vitamin B12, and vitamin D.
- Check to be sure a child is ingesting a variety of calcium sources (e.g., green leafy vegetables, milk products) because calcium is very important for bone growth.
- Vitamin D is found in fortified cereals and milk.
- Vitamin B12 is found almost exclusively in animal products, so a child on a vegetarian intake may need a supplemental source.
Promoting Preschooler Development in Daily Activities
- Dressing: Many 3-year-olds and most 4-year-olds can dress themselves except for difficult buttons, although conflict may occur over what the child will wear. Preschoolers prefer bright colors or prints and so may select items that are appealing in color rather than matching. As with other preschool activities, however, children need the experience of choosing their own clothes.
- Sleep: Many toddlers, who go through a typical negative phase, resist taking naps no matter how tired they are. Preschoolers, however, are more aware of their needs; when they are tired, they often curl up on a couch or soft chair and fall asleep. Afternoon naps may be given up, especially for those who attend afternoon child care or preschool. Afternoon naps may result in some difficulty going to sleep at the usual bedtime established at home.
- On some occasions, even though they may be tired, children in this age group may refuse to go to sleep because of fear of the dark (i.e., magical thinking) and may wake at night terrified by a bad dream. A night-light may be beneficial. Stimuli for fear such as frightening stories or TV watching prior to bedtime should be removed.
- Exercise: The preschool period is an active phase, so preschool play tends to be vigorous. Roughhousing helps relieve tension and should be allowed as long as it does not become destructive. In addition, preschoolers love time-honored games such as ring around-the-rosy, London Bridge, or other more structured games they were not ready for as toddlers. Promoting these types of active games and reducing television watching can be steps toward helping children develop motor skills as well as prevent childhood obesity.
- Hygiene: Preschoolers can wash and dry their hands adequately if the faucet is regulated (<120°F) for them (so they do not scald themselves with hot water).
- Additional products should not be added to bathwater to prevent irritation, especially for girls.
- Drowning remains a source of injury. Do not leave preschoolers unsupervised at bath time. They may also add more hot water to the tub, which can result in scalding.
- Dental Hygiene: If independent toothbrushing was not started as a daily practice during the toddler years, it should be started during preschool. One good toothbrushing period a day is often more effective than more frequent half-hearted attempts.
- Although many preschoolers do well brushing their own teeth, parents must check that all tooth surfaces have been cleaned. Parents should also floss the child’s teeth because this is a skill beyond a preschooler’s motor ability.
- Preschoolers should continue to drink fluoridated water or receive a prescribed oral fluoride supplement if fluoride is not provided in the water supply.
- A first visit to a dentist should be arranged no later than 2 years of age for an evaluation of tooth formation because deciduous (baby) teeth must be preserved to protect the dental arch. Dental services can be performed at 3 years of age.
- Teeth grinding (bruxism) may begin at this age as a way of “letting go,” similar to body rocking, which children do for a short time each night before falling asleep. Children who grind their teeth extensively may have greater than average anxiety. This may also be a result of jaw spasticity in children with cerebral palsy. If grinding is extensive, the crowns of the teeth can actually become abraded. The condition can advance to such an extent that tooth nerves become exposed and painful. Referral to a pediatric dentist is required if damage is evident.
Parental Concerns Associated with the Preschool Period
- Questions: Answering a preschooler’s questions can be difficult, because the questions are frequently philosophical, not fact finding such as, “Why is grass green?” A child may listen to an explanation of chlorophyll but then repeat the question, regardless of the clarity of the explanation, because the parent underestimated the depth of the question. The child did not want to know what makes grass green but why, philosophically, it is not red, blue, or yellow. The obvious answer to that is “I don’t know.” Parents who are confident can give this answer without feeling threatened. Parents who are less sure of themselves may feel extremely uncomfortable when they realize they do not know the answer to what a 4-year-old is asking.
- Discipline: Preschoolers have definite opinions on things such as what they want to eat, where they want to go, and what they want to wear, and these opinions may bring them into opposition with parents. A major parental responsibility when this happens is to guide a child through these struggles without discouraging the child’s right to have an opinion. A “time-out” is a useful technique for parents to correct behavior throughout the preschool years, as it was during toddlerhood. Time-out periods should be as many minutes long as the child is old, so 3 to 5 minutes is appropriate for preschoolers.
- Common Health Problems: Mortality in preschool years is low and becoming lower every year with advances in medicine. The major cause of death in preschoolers are automobile accidents, followed by poisoning and falls. Although major illnesses are few, the number of minor illnesses, such as common colds and ear infections, are high.
- Assess to be certain such constant illness is not causing parents to perceive a child as sickly or not able to cope with everyday life so they don’t begin to discourage independence in favor of overprotection. As parents become more experienced in handling these conditions, their perception of whether an illness is serious or not and their ability to cope with them will change.
- A child whose parents smoke have a higher incidence of ear (otitis media) and respiratory infections than others.
- A child who attends child care or preschool programs also have an increased incidence of gastrointestinal disturbances (vomiting and diarrhea) and upper respiratory infections from the exposure to other children.
- Urinary tract infections tend to occur with a high frequency in preschool-age girls.
- Fears of the Preschooler: the preschooler’s highly active imagination leads to a number of fears. These can rise in incidence when combined with the stress of an illness, hospitalization, or unsafe conditions in the child’s community.
- Fear of the Dark: They may be reluctant to go to bed or go back to sleep by themselves unless a light is left turned on or a parent sits nearby. If parents are prepared for this fear and understand it is a phase of growth, they are better able to cope with it. It is generally helpful if they monitor the stimuli their children are exposed to, especially around bedtime. This includes television, adult discussions, and frightening stories. A night light is an effective intervention.
- Fear of Mutilation: Intense fear is felt towards even simple injuries such as falling and scraping a knee or having a needle inserted for an immunization. Part of this fear arises because preschoolers do not know which body parts are essential and which ones—like an inch of scraped skin—can be easily replaced. Boys develop a fear of castration. Any procedure that feels invasive is disliked. They need good explanations of the limits of healthcare procedures, such as clarifying a tympanic thermometer does not hurt or a finger prick heals quickly as well as distraction techniques in order to feel safe.
- Fear of Separation or Abandonment: Their sense of time and distance is still so limited that they cannot be comforted by assurances such as “Mommy will pick you up from preschool at noon” or “I work only a block away” is not reassuring. Relating time and space to something a child knows better, such as meals, television shows, or a friend’s house, is more effective (e.g., “I will pick you up after you finish your snacks.“)
- Changes in Behavior: A combination of a keen imagination and immature reasoning results in a number of other common behavior variations in preschoolers.
- Telling Tall Tales: stretching stories is commonly encountered in preschoolers. They may reply to questions with an “exciting” answer because they expect the person asking them to want an interesting answer, rather than simply to lie. Caution them not to encourage this kind of storytelling but instead help the child separate fact from fiction by saying, “That’s a good story, but now, tell me what really happened.” This conveys the idea that the child has not told the truth, yet does not squash imagination or initiative.
- Imaginary Friends: Although imaginary friends are a normal, creative part of the preschool years and can be invented by children who are surrounded by real playmates as well as by those who have few friends, parents may find them disconcerting. Let parents know that, as long as the child has exposure to real playmates and imaginary playmates do not take center stage in children’s lives or prevent them from socializing with other children, they should not pose a problem. In the meantime, pretend friends can encourage language development, may provide an outlet for a child to express innermost feelings, or serve as a handy scapegoat for behavior about which a child has some conflict.
- Difficulty Sharing: Sharing is a concept that first comes to be understood around the age of 3 years. Before this, children engage in parallel play. Around 3 years of age, children begin to understand some things are theirs, some belong to others, and some can belong to both. For the first time, they can stand in line to wait for a drink, take turns using a shovel at a sandbox, and share a box of crayons. Sharing does not come easily. Defining limits and exposing children to these three categories (i.e., mine, yours, ours) helps them determine which objects belong to which category.
- Regression: Some preschoolers, generally in relation to stress, revert to behavior they previously outgrew, such as thumb-sucking, negativism, loss of bladder control, and inability to separate from their parents. Although the stress that causes this may take many forms, it is usually the result of such things as a new baby in the family, a new school experience, seeing frightening and graphic television news or programming, stress in the home from financial or marital difficulties, or separation caused by hospitalization. This is normal. Obviously, removing the stress is the best way to help a child discontinue this behavior.
- Sibling Rivalry: Jealousy of a brother or sister may first become evident during the preschool period because this is the first time children have enough vocabulary to express how they feel (i.e., know a name to call) and partly because preschoolers are more aware of family roles and how responsibilities at home are divided. A firstborn child often becomes a “trial run” for parents to test the level of responsibility allowable for a child. This results in second children being allowed privileges that were not allowed for the first child. Children as young as preschool can tell when a younger sibling is allowed behavior that is not tolerated in them. They are little appeased by the explanation, “Your brother is just a baby.” Remind preschoolers that there are things they can do that a younger sibling is not allowed to do and supply them with a private drawer or box for their things that others are not allowed to access.
- Sex Education: During the preschool age, children become acutely aware of the difference between boys and girls. Possibly, this is a normal progression in development, and, possibly, this may be the first time they are exposed to the genitalia of the opposite sex as they watch while a new brother or sister has a diaper changed, they see other children using the bathroom at a preschool, or they see a parent nude.
- Preschoolers’ questions about genital organs are simple and fact finding; for example, “Why does James look like that?” or “How does Jasmine pee?” Explanations should be just as simple: “Boys look different from girls. The different part is called a penis.” It is important that parents do not convey that these body parts are never to be talked about so they leave an open line of communication for sexual questions.
- It is common for preschoolers to engage in masturbation while watching TV or before they fall asleep at night. The frequency of this may increase under stress, as does thumb-sucking. If observing a child doing this bothers parents, suggest they explain certain things are done in some places but not in others. Unnecessary attention to the activity can increase anxiety and cause increased, not decreased, activity.
- Broken Fluency: Developing language is such a complicated process that children from 2 to 6 years of age typically have some speech difficulty. A child may begin to repeat words or syllables, saying, “I-I-I want a n-n-new spoon-spoon-spoon.” This is called broken fluency (repetition and prolongation of sounds, syllables, and words). It is often referred to as secondary stuttering because the child began to speak without this problem and then, during the preschool years, develops it. Unlike in adults, the child is not aware that they are not being fluent unless it is brought to their attention. This is a part of normal development and will pass. Resolution may accelerated by avoiding making the child conscious of their broken fluency, speaking slowly to role model for the child, and not forcing the child to speak when do not wish to.
Summary of Preschooler Growth and Developmental Milestones
| Age (in Years) | Fine Motor Skills | Gross Motor Skills | Language | Play |
|---|---|---|---|---|
| 3 | Undresses self; stacks tower of blocks; draws a cross | Runs; alternates feet on stairs; rides tricycle; stands on one foot | Vocabulary of 900 words | Able to take turns; very imaginative |
| 4 | Can do simple buttons | Constantly in motion; jumps; skips | Vocabulary of 1,500 words | Pretending is major activity |
| 5 | Can draw a six part figure; can lace shoes | Throws overhand | Vocabulary of 2,100 words | Likes games with numbers or letters |
Nursing Care of a Family with a School-Age Child
The term “school age” refers to children between the ages of 6 and 12 years. Although these years represent a time of slow physical growth, the school-age child’s cognitive growth and development continue to proceed at rapid rates. The school-age period is a relatively long time span, and even though growth is slow, children grow and develop extensively during this time period.
Physical Growth
- Weight and Height: The average annual weight gain for a school-age child is approximately 3 to 5 lb (1.3 to 2.2 kg); the increase in height is 1 to 2 in. (2.5 to 5 cm). Children who did not lose a lordosis and knock-kneed appearance during the preschool period lose this now.
- By 10 years of age, brain growth is complete, so fine motor coordination becomes refined. As the eye globe reaches its final shape at about this same time, an adult vision level is achieved.
- If the eruption of permanent teeth and growth of the jaw do not correlate with final head growth, malocclusion with teeth malalignment may be present.
- The left ventricle of the heart enlarges to be strong enough to pump blood to the growing body. Innocent heart murmurs may become apparent due to this extra blood crossing heart valves. The pulse rate decreases to 70 to 80 beats/min; blood pressure rises to about 112/60 mmHg.
- At a set point in brain maturity, the hypothalamus transmits an enzyme to the anterior pituitary gland to begin production of gonadotropic hormones, which then activate changes in the testes and ovaries to cause puberty.
- Teeth: deciduous teeth are lost and permanent teeth erupt during the school-age period. Because of this, the average child gains 28 teeth between 6 and 12 years of age: the central and lateral incisors; first, second, and third cuspids; and first and second molars.
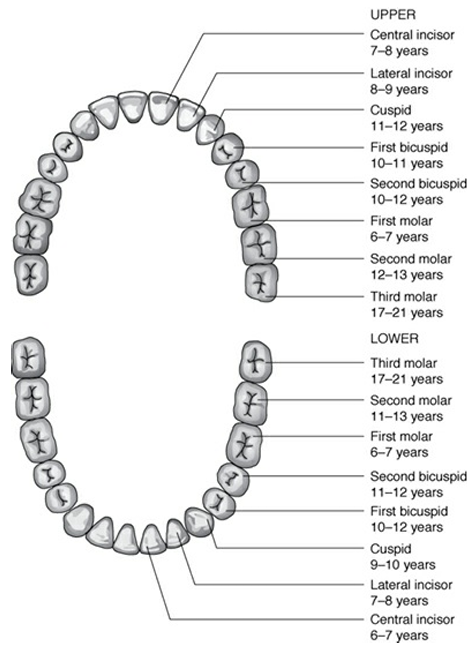
Puberty
| Age (in Years) | Boys | Girls |
|---|---|---|
| 9–11 | Prepubertal weight gain occurs. | Breasts: elevation of papilla with breast bud formation; areolar diameter enlarges. |
| 11–12 | Sparse growth of straight, downy, slightly pigmented hair at base of penis. Scrotum becomes textured; growth of penis and testes begins. Sebaceous gland secretion increases. Perspiration increases. | Straight hair along the labia; vaginal epithelium becomes cornified. pH of vaginal secretions becomes acidic; slight mucous vaginal discharge is present. Sebaceous gland secretion increases. Perspiration increases. Dramatic growth spurt. |
| 12–13 | Pubic hair present across pubis. Penis lengthens. Dramatic linear growth spurt. Breast enlargement may occur. | Pubic hair grows darker; spreads over entire pubis. Breasts enlarge, still no protrusion of nipples. Axillary hair present. Menarche occurs. |
Timing of the onset of puberty varies widely, between 8 and 14 years of age, partly due to genetic and cultural differences, and is rated according to Tanner stages. The length of time it takes to pass through puberty until sexual maturity is complete also varies. Sexual maturation in girls usually occurs between the years of 12 and 18; in boys, between 14 and 20 years.
The changes in physical appearance that come with puberty can lead to concerns for both children and their parents. The school-age period is a time for parents to discuss with children the physical changes that will occur and the sexual responsibility these changes dictate.
- Concerns of Girls:
- Prepubertal girls are usually taller than preadolescent boys because their typical growth spurt begins earlier. This may cause concern, especially in a culture in which boys are expected to be taller than girls.
- A girl may also notice changes in their pelvic contour and realizes her hips are becoming broader. She may misinterpret this as a gain in weight and attempt a crash diet. This is a normal part of an adult female profile.
- Girls may also be conscious of breast development. Early breast development may lead to slouching or wearing of loose clothing to hide the size of her breasts, while others may wonder whether their breasts are going to develop enough.
- Early preparation for menstruation is also an important preparation for future childbearing and for a girl’s concept of herself as a woman. A girl who is told menstruation is a normal function that occurs every month in all healthy women has a different attitude toward her body than a girl who wakes up one morning to find blood on her pajamas and is told bluntly, “You’d better get used to that. You’ll have to put up with it for the rest of your life.”
- Concerns of Boys:
- Just as girls become keenly aware of breast development, boys become aware of increasing genital size. If they do not know testicular development precedes penis growth, they can worry that their growth will be inadequate.
- Hypertrophy of breast tissue (gynecomastia) can occur in prepubescent boys, most often in those who are obese. He can be assured that this is a transitory phenomenon and, although it makes him self-conscious, will fade as soon as his male hormones become more mature and active.
- Some boys can also become concerned because although they have pubic hair, they cannot yet grow a beard or do not have chest hair, which are outward, easily recognized signs of maturity. You can assure them that pubic hair normally appears first and that chest and facial hair may not grow until several years later.
- As increased seminal fluid begins to be produced, boys begin to notice ejaculation during sleep, termed nocturnal emissions. This is in no way debilitating or a sign of premature ejaculation, which are both common myths associated with nocturnal emissions.
- In both sexes, puberty brings changes in the sebaceous glands. Under the influence of androgen, glands become more active, setting the stage for acne.
Gross Motor Development
At the beginning of the school age period (age 6 years), children endlessly jump, tumble, skip, and hop. They have enough coordination to walk a straight line, many can ride a bicycle, and they learn to skip rope with practice.
| Age (in Years) | Physical Development | Psychosocial and Cognitive Development |
|---|---|---|
| 6 | A year of constant motion; skipping is a new skill; first molars erupt. | First-grade teacher becomes authority figure; adjustment to all-day school may be difficult and may lead to nervous manifestations of fingernail biting, etc. Defines words by their use (e.g., a key is to unlock a door, not a metal object). |
| 7 | Central incisors erupt; difference between sexes becomes apparent in play (e.g., video games vs. dolls); spends time in quiet play. | A quiet year; striving for perfection leads to this year being called an eraser year. Learns conservation (e.g., water poured from tall container to a wide, flat one is the same amount of water); can tell time; can make simple change. |
| 8 | Coordination definitely improved; eyesight fully develops; playing with friends becomes important. | “Best friends” develop; whispering and giggling begin; can write in cursive as well as print; understands concepts of past, present, and future. |
| 9 | All activities done with friends | Friend or club age; a 9-year-old club is formed to spite someone, has secret codes, is all boy or all girl; clubs disband and reform quickly. |
| 10 | Coordination improves. | Ready for camp away from home; collecting age; likes rules; ready for competitive games. |
| 11 | Active, but awkward and ungainly | Insecure with members of opposite sex; repeats off-color jokes. |
| 12 | Coordination improves. | A sense of humor is present; is social and cooperative. |
Fine Motor Development
- Six-year-olds can easily tie their shoelaces. They can cut and paste well and draw a person with good detail. They can print, although they may routinely reverse letters.
- Seven-year-olds concentrate on fine motor skills even more than they did the year before. This has been called the “eraser year” because children are never quite content with what they have done. They set too high a standard for themselves and then have difficulty performing at that level.
- By 8 years of age, children’s eyes are developed enough so they can read regular size type. This can make reading a greater pleasure and school more enjoyable. Eight-year-olds are able to write script in addition to print. They enjoy showing off this new skill in cards, letters, or projects.
- By age 9 years, their writing begins to look mature and less awkward.
- Older school-age children begin to evaluate their teachers’ ability and may perform at varying levels depending on each teacher’s expectations. The middle school curriculum involves more challenging science and mathematics courses than previously and includes good literature. This may be a child’s first exposure to reading as a fulfilling and worthwhile experience rather than just as an assignment and may be the time a child is “turned on” to reading.
Play
| Age (in Years) | Physical Development |
|---|---|
| 6 | Reading becomes enjoyable. Children may start spending quiet time with books. Many children spend hours playing increasingly challenging video games. |
| 7 | Children require more props for play than when they were younger, such as for roleplay. This coincides with a decline in imaginative play. Children begin to prefer teenage dolls if they play with dolls, and their coordination is good enough that they can button the miniature dresses and pull on the tiny boots. Collecting items becomes interesting, usually for quantity rather than the type of item itself. |
| 8 | Collecting becomes more structured; time is spent sorting and cataloging. Most girls and boys of this age also enjoy helping in the kitchen with jobs such as making cookies and salads or frosting cakes. They start to be more involved in simple science projects and experiments. Children like table games but hate to lose, so they tend to avoid competitive games. They may change the rules in the middle of a game to keep from losing. |
| 9 | Nine-year-olds play hard. They squeeze in play when possible, and may defer sleep to play “just one more game”. Play is rough. Many schools begin music lessons for children at about 9 years of age. Children do well if others in their group are taking similar lessons. Talent for music or art becomes evident, and children respond with new interest in school or wherever they are exposed to these arts. Nine years of age is also a time when children use social media. This is an activity parents need to supervise as they may not realize that their accounts are available to the public and potential child predators. |
| 10 | Many spend most of their time playing screen games. Slumber parties and campouts become increasingly popular. |
| 11–12 | Dancing and playing table games; they are accommodating enough again to be able to play with younger siblings who need the rules modified to their advantage. Time with friends is often spent just talking. |
Language Development
- Six-year-olds talk in full sentences, using language easily and with meaning. They no longer sound as though talking is an experiment but appear to have incorporated language permanently. They still define objects by their use (e.g., a key is to unlock a door, a fork is to eat with).
- Most seven-year-olds are able to tell time in hours and months. They may struggle with phrases such as “half past” and “quarter to,” especially with the prevalence of digital clocks. They are also able to add and subtract and make simple change, allowing them to make simple purchases.
- Nine-year-olds discover “dirty” jokes. They use swear words to express anger to just to show other children that they are growing up. Intense fascination for “bathroom language” may appear again, as they did during the preschool years.
- By 12 years of age, children can carry on an adult conversation, although stories are limited because of a lack of experience.
Emotional Development
Ideally, children enter the school-age period with the ability to trust others (Trust vs. Mistrust) and with a sense of respect for their own worth. They can accomplish small tasks independently because they have gained a sense of autonomy (Autonomy vs. Shame and Doubt). They should have practiced or mimicked adult roles, learned to share, discovered that learning is an adventure, and grasped the idea that doing things is more important and more rewarding than watching things being done (initiative) (Initiative vs. Guilt). These are all developmental tasks experienced by the child from infancy to preschool age.
The school-age child’s new developmental step is learning a sense of industry or accomplishment. If gaining a sense of initiative can be defined as learning how to do thing, then gaining a sense of industry is learning how to do things well. If children are prevented from achieving a sense of industry or do not receive rewards for accomplishment, they can develop a feeling of inferiority or become convinced they cannot do things they actually can do. These children can have difficulty tackling new situations later in life because they cannot envision how they will be successful in handling them. This can result in frustration in school or work activities.
The questions a preschool child asks reflect curiosity, such as “how,” “why,” and “what.” During the early school years, children concentrate their questions on the “how” of tasks: “Is this the right way to do this?” “Am I making this right?” and “Is this good?” Often, school-age children will comment, “I can’t do anything right” because their craft project falls short of expectations. School-age children need reassurance that they are doing things correctly, and this reassurance is best if it comes immediately after a task is completed.
| Age (in Years) | Socialization |
|---|---|
| 6 | Plays in groups; prefers one-to-one contact when tired. |
| 7 | Increasingly aware of family roles and responsibility. Promises are viewed as definite, firm commitments and must be kept. Children this age tattle because they have such a strong sense of justice. |
| 8 | Eight-year-olds actively seek the company of other children, primarily for same-sex peers. Children often have close boy friends or girl friends. |
| 9 | Children are ready for activities away from home, such as a week at camp. They can take care of their own needs and are mature enough to be separated from their parents for this length of time. |
| 10 | Although 10-year-olds enjoy groups, they also enjoy privacy. They like having their own bedroom or at least their own dresser, where they can store a collection and know it is free from parents’ or siblings’ eyes. One of the best gifts for a 10-year-old is a box that locks. |
| 11 | Girls become increasingly interested in boys and vice versa by 11 years of age. They remain awkward, and require practice to become comfortable in forming relationships with the opposite sex. |
| 12 | Children feel more comfortable in social situations than they did the year before. Boys experience erections on small provocation and so may feel uncomfortable being pushed into boy–girl situations until they learn how to better control their bodies. |
Cognitive Development
The age from 5 to 11 years is a transitional stage where children undergo a shift from the preoperational thought they used as preschoolers to concrete operational thought or the ability to reason through any problem they can actually visualize. Children can use concrete operational thought because they learn several new concepts during school age, such as:
- Decentering, the ability to project one’s self into other people’s situations and see the world from their viewpoint rather than focusing only on their own view. Decentering enables a school-age child to feel compassion for others, which was not possible in younger years.
- Accommodation, the ability to adapt thought processes to fit what is perceived such as understanding that there can be more than one reason for other people’s actions. A preschooler might expect to see the same nurse in the morning who was there the evening before, whereas a school-age child will understand that different nurses work different shifts.
- Conservation, the ability to appreciate that a change in shape does not necessarily mean a change in size. If you pour 30 ml of cough medicine from a thin glass to a wide one, the preschooler will say that one glass holds more than the other; a school-age child will know that both glasses hold an equal amount. Because understanding the principle of conservation is possible, a school-age child is not fooled by perceptions as often as before.
- Class inclusion, the ability to understand that objects can belong to more than one classification. A preschooler is able to categorize items in only one way, for example, stones and shells are found at the beach; a school-age child can categorize them in many ways such as by different materials or by a difference in sizes and shapes, not just that they are found at the beach. The ability to classify objects leads to the collecting activities of the school-age period.
Moral and Spiritual Development
School-age children begin to mature in terms of moral development as they enter a stage of preconventional reasoning, sometimes as early as 5 years of age. During this stage, if asked, “Why is it wrong to steal from your neighbor?” school-age children will answer, “The police say it’s wrong,” or “Because if you do, you’ll go to jail.” They concentrate on “niceness” or “fairness” and cannot see yet that stealing hurts their neighbor, the highest level of moral reasoning. Because they are still limited in their ability to understand others’ views, they may interpret something as being right because it is good for them, not because it is right for humanity as a whole.
Nursing Roles in Health Promotion During School Age
1894