References:
- Wong’s Nursing Care of Infants and Children, 11th Edition, ISBN 978-0-323-54939-4, by Marilyn J. Hockenberry, David Wilson, and Cheryl C. Rodgers (pp. 1159-1165)
Hydrocephalus is a condition caused by an imbalance in the production and absorption of CSF in the ventricular system. The underlying problem is either (1) impaired absorption of CSF fluid (nonobstructive or communicating hydrocephalus) or (2) obstruction to the flow of CSF through the ventricular system (obstructive or noncommunicating hydrocephalus).
In both occurrences, the imbalance of secretion and absorption causes an increased accumulation of CSF in the ventricles, which become dilated (ventriculomegaly) and compress the brain tissue against the surrounding rigid cranium.
- If this occurs before the fusion of the cranial sutures, it causes enlargement of the skull and dilation of the ventricles.
- In children younger than 12 years old, previously closed sutures, especially the sagittal suture, may become diastatic or opened.
- After 12 years old, the sutures are fused and will not open.
Pathophysiology
The two mechanisms by which CSF is formed are secretion by the choroid plexuses and lymphatic-like drainage by the extracellular fluid of the brain. CSF circulates throughout the ventricular system and is then absorbed within the subarachnoid spaces by a mechanism that is not entirely clear.
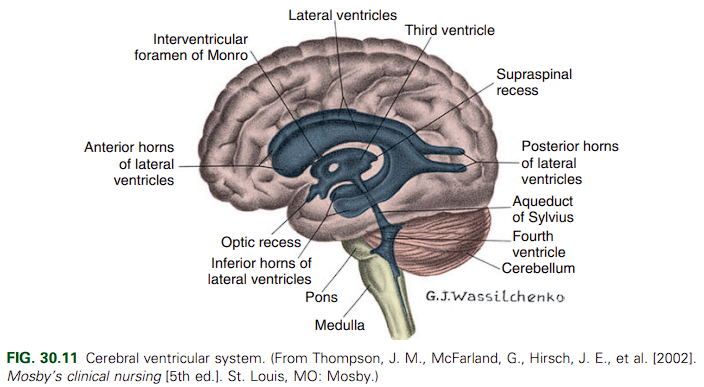
Ventricular Circulation
The fluid flows from the lateral ventricles through the foramen of Monro to the third ventricle, where it combines with fluid secreted into the third ventricle. From there CSF flows through the aqueduct of Sylvius into the fourth ventricle, where more fluid is formed; it then leaves the fourth ventricle by way of the lateral foramen of Luschka and the midline foramen of Magendie and flows into the cisterna magna. From the cisterna magna, CSF flows to the cerebral and cerebellar subarachnoid spaces where it is absorbed. A large portion is absorbed through the arachnoid villi, but the sinuses, veins, brain substance, and dura also participate in absorption.
The causes of hydrocephalus are varied and include either congenital or acquired conditions such as intraventricular hemorrhage, tumor, CSF infection, or head injury.
- Congenital developmental defects (e.g., Chiari malformation, aqueductal stenosis, aqueductal gliosis, and atresia of the foramina of Luschkla and Magendie [Dandy-Walker malformation]) make up most cases of hydrocephalus.
- Acquired conditions (e.g., intraventricular hemorrhage, tumor, meningitis, encephalitis, head trauma/injury)
In particular, a Chiari II malformation (the lower cerebellum and brain stem protrude into the spinal canal through an enlarged foramen magnum) is almost exclusively associated with myelomeningocele, which is often associated with hydrocephalus; so often that all infants with myelomeningocele should be observed for the development of hydrocephalus.
Clinical Manifestations
The three factors that influence the clinical picture in hydrocephalus are the acuity of onset, timing of onset, and associated structural malformations. In infancy, before closure of the cranial sutures, head enlargement (increasing occipitofrontal circumference [OFC]) is the predominant sign. The signs and symptoms in early to late childhood are caused by increased ICP, and specific manifestations appear related to the location of the lesion in obstructive hydrocephalus.
- Infancy: the head grows at an abnormal rate, although the first signs may be bulging fontanels with or without head enlargement.
- The anterior fontanel is tense, often bulging, and nonpulsatile.
- Scalp veins are dilated, especially when the infant cries.
- With the increase in intracranial volume, the bones of the skull become thin and the sutures become palpably separated to produce the cracked-pot sound (Macewen sign) on percussion of the skull.
- In severe cases, there may be frontal protrusion, or frontal bossing, with depressed eyes, and the eyes may be rotated downward, producing a setting-sun sign, in which the sclera may be visible above the iris. Pupils are sluggish, with unequal response to light.
- Increased ICP will cause irritability, lethargy, poor feeding, changes in level of consciousness, opisthotonos (often extreme), and lower extremity spasticity. Picking up the infant or rocking the infant will cause crying, and lying still will quiet the infant.
- Early infantile reflexes may persist, and normally expected responses may not appear, indicating failure in the development of normal cortical inhibition.
- Infants with Chiari malformations may exhibit behaviors that reflect cranial nerve dysfunction as a result of brainstem compression, including swallowing difficulties, stridor, apnea, aspiration, respiratory difficulties, and arm weakness.
- If hydrocephalus is allowed to progress, development of lower brainstem functions is disrupted, as manifested by difficulty in sucking and feeding and a shrill, brief, high-pitched cry. Eventually the skull becomes enlarged, and the cortex is destroyed. If the hydrocephalus is rapidly progressive, symptoms may include emesis, somnolence, seizures, and cardiopulmonary distress.
- Childhood: the signs and symptoms in early to late childhood are caused by increased ICP, and specific manifestations are related to the location of the focal lesion. Most commonly resulting from posterior fossa neoplasms and aqueduct stenosis, the clinical manifestations are primarily those associated with space-occupying lesions (i.e., headache on awakening with improvement after emesis, papilledema, strabismus, and extrapyramidal tract signs such as ataxia. As with infants, the child is irritable, lethargic, apathetic, confused, and often incoherent.
- In one of the congenital defects with later onset (by age 3 months), the Dandy-Walker syndrome, characteristic manifestations are a bulging occiput, nystagmus, ataxia, and cranial nerve palsies.
- Chiari malformation in children over 3 years of age are related to spinal cord dysfunction rather than brainstem compression as observed in infants. Scoliosis proximal to the level of the myelomeningocele (usually associated with Chiari malformation) and development of upper extremity spasticity, which may progress to weakness and atrophy, are common. Cranial nerve deficits are rare.
Diagnostic Evaluation
Antenatal diagnosis of fetal ventriculomegaly, which is associated with postnatal hydrocephalus, is possible with fetal ultrasonography as early as 14 to 15 weeks of gestation, often followed by fetal MRI.
- In infancy, diagnosis of hydrocephalus is based on head circumference that crosses one or more percentile lines on the head measurement chart within a period of 2 to 4 weeks and on associated neurologic signs that are progressive. Routine daily head circumference measurements are carried out in infants with myelomeningocele, hemorrhage, or intrauterine viral or CNS infections.
- The primary diagnostic tools for detecting hydrocephalus in older infants and children are CT and MRI.
Therapeutic Management
The treatment of hydrocephalus is directed toward relief of ventricular pressure, treatment of the cause of the ventriculomegaly, treatment of associated complications, and management of problems related to the effect of the disorder on psychomotor development. The treatment is, with few exceptions, surgical.
- Direct removal of an obstruction (neoplasm, cyst, hematoma), or rarely choroid plexus extirpation to reduce fluid production.
- Shunt procedures are necessary for most children to drain the CSF from the ventricles to an extracranial compartment, usually the peritoneum. The standard procedure for many years has been the ventriculoperitoneal (VP) shunt, especially in neonates and young infants.
- Most shunt systems consist of a ventricular catheter, a flush pump, a unidirectional flow valve, and a distal catheter. All are radiopaque for easy visualization after placement, and all are tested for accuracy before insertion.
- A reservoir is frequently added to allow direct access to the ventricular system for administration of medications and removal of fluid.
- In all models the valves are designed to open at a predetermined intraventricular pressure and close when the pressure falls below that level, thus preventing backflow of fluid.
- All shunts require revision as the body becomes larger.
- Endoscopic third ventriculostomy (ETV) for obstructive hydrocephalus is, on the short term, comparable to VP shunting. Long-term outcomes need to be studied. The use of ETV eliminates the risk of infection and shunt failure.
Complications
The major complications of VP shunts are infection and malfunction. All shunts are subject to mechanical difficulties, such as kinking, plugging, or separation and migration of tubing. Malfunction is most often caused by mechanical obstruction either within the ventricles from particulate matter (tissue or exudate) or at the distal end from thrombosis or displacement as a result of growth.
- Functional obstruction of a shunt’s antisiphon device remains a common complication. About 22% of shunt failures are reported within the first 90 days, the majority of these within the first month.
- The child with a shunt obstruction often is seen in an emergency visit with clinical manifestations of increased ICP, such as nausea, vomiting, irritability, and a bulging fontanel, that is frequently accompanied by worsening neurologic status.
- One of the most common and serious complications, shunt infection, can occur at any time, but the period of greatest risk is within the first month after placement. This may include sepsis, bacterial endocarditis, wound infection, shunt nephritis, meningitis, and ventriculitis and may be a result of intercurrent infections at the time of shunt placement.
Nursing Care Management
The infant with suspected or confirmed hydrocephalus is observed carefully for signs of increasing ventricular size and increasing ICP.
- In infants the head is measured daily at the point of largest measurement—the occipital frontal circumference (OFC).
- Fontanels and suture lines are palpated for size, signs of bulging, tenseness, and separation.
- The most valuable indicators of increasing ICP are an alteration in the child’s level of consciousness, complaint of headache, and changes in interaction with the environment. Changes are identified by observing and comparing present behavior with customary behavior obtained through a detailed history and a baseline assessment.
- Prepare the child for diagnostic tests such as MRI or a CT scan. The nurse also assists with procedures such as a ventricular tap, which is often performed to relieve excessive pressure and to obtain CSF during the preoperative period.
- Postoperative Care: the child is positioned flat carefully on the unoperated side to prevent pressure on the shunt valve, and prevent rapid reduction of intracranial fluid due to gravity. The surgeon may specify the position to maintain and the extent of activity allowed.
- Continue monitoring for signs of increased ICP that indicate obstruction of the shunt— pupil dilation from compression of the oculomotor nerve, variable blood pressure.
- The nurse also observes for abdominal distention and constipation because CSF may cause peritonitis or a postoperative ileus as a complication of distal catheter placement.
- Infections are the greatest hazard. Usual manifestations of CSF infection are monitored, including elevated temperature, poor feeding, vomiting, decreased responsiveness, and seizure activity. there may be signs of local inflammation at the operative sites and along the shunt tract.
- Provide Family Support. Inform them of the disease, diagnostic procedures, and surgical procedures. For discharge, the parents are instructed on how to recognize signs that indicate shunt malfunction or infection.
- Educate the parents on which activities are allowed. Contact sports are usually prohibited. Other sports such as swimming, soccer, and track are acceptable and even encouraged for the child’s physical and emotional health.