References:
- Wong’s Nursing Care of Infants and Children, 11th Edition, ISBN 978-0-323-54939-4, by Marilyn J. Hockenberry, David Wilson, and Cheryl C. Rodgers (pp. 795-799)
Nephrotic syndrome is the most common presentation of glomerular injury in children. It is defined as massive proteinuria, hypoalbuminemia, hyperlipidemia, and edema and is a clinical manifestation of a large number of distinct glomerular disorders in which increased glomerular permeability to plasma protein results in massive urinary protein loss.
- Minimal Change Nephrotic Syndrome makes up ~80% of cases of nephrotic syndrome in children. MCNS can be seen at any age but is predominantly a disease of the preschool child. It is unusual after 8 years of age. A nonspecific, often viral upper respiratory tract infection, often precedes the manifestations by 4 to 8 days but is considered to be a precipitating factor than a cause.
- Secondary Nephrotic Syndrome is glomerular damage due to known or presumed cause, such as acute glomerulonephritis or chronic glomerulonephritis. It may also result from collagen vascular diseases (disseminated lupus erythematosus, anaphylactoid purpura), toxicity (drugs, stings, venom).
- Nephrotic Syndrome is the major presenting symptom of pediatric clients with acquired immunodeficiency syndrome.
- Congenital Nephrotic Syndrome-Finnish Type is an autosomal recessive form of nephrotic syndrome. These children are small for gestational age, and manifest proteinuria and edema within the first few days to months of age. Usual therapy is not effective in these cases. Therapy is required to prevent death within the first year or two of life, including IV administration of albumin, nutritional support, dialysis, or a kidney transplant.
The discussion will be focusing on the most common form of nephrotic syndrome— MCNS.
Pathophysiology
- A metabolic, biochemical, or physiochemical disturbance in the basement membrane of the glomeruli may lead to increased permeability to protein, but the causes and mechanisms are only speculative.
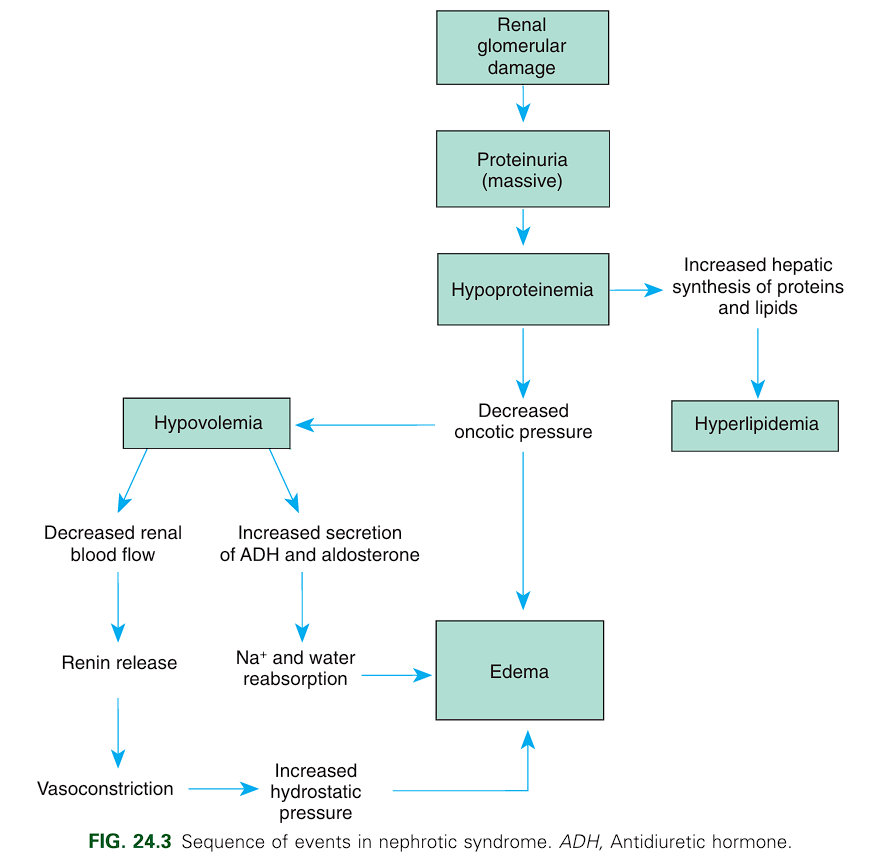
- The glomerular membrane, normally impermeable to albumin and other large proteins, becomes permeable to proteins. Albumin leaks into urine, producing massive proteinuria and hypoalbuminemia.
- Colloidal pressure (COP) decreases in the capillaries from the reduced protein concentration. Hydrostatic pressure exceeds the pull of the COP, and fluid accumulates in the interstitial spaces and body cavities (edema), particularly the abdominal cavity (ascites).
- The shift of fluid from the plasma reduces the vascular fluid volume (hypovolemia), which in turn activates the renin-angiotensin system and the secretion of antidiuretic hormone and aldosterone. Fluids and sodium are retained as an attempt to increase intravascular volume.
- The elevation of serum cholesterol, phospholipids, and triglycerides is not fully understood. However, it is in response to hypoproteinemia that the liver begins lipoprotein (LDL) synthesis, which eventually results in hyperlipidemia.
Clinical Manifestations
A previously well child begins to gain weight, which progresses over a period of days or weeks. Most of the clinical manifestations center around edema.
- Puffiness of the face, especially around the eyes, is apparent on rising in the morning but subsides during the day, when swelling of the abdomen, genitalia, and lower extremities is more prominent.
- Generalized edema (anasarca) may develop gradually or rapidly.
- Edema of the intestinal mucosa may cause diarrhea, loss of appetite, and poor intestinal absorption.
- The volume of urine is decreased, and it appears darkly opalescent and frothy.
- Severe edema causes the skin to appear with extreme skin pallor and even skin breakdown.
- The child may be irritable and more easily fatigued or lethargic but does not appear seriously ill.
- Muehrcke lines—white lines parallel to the lunula, is caused by prolonged hypoalbuminemia.
The child is more susceptible to infections, particularly of cellulitis, pneumonia, peritonitis, or sepsis.
Rarely, significant or persistent hypertension, gross or persistent hematuria, or significant or persistent azotemia also occur.
Diagnostic Evaluation
Diagnosis of MCNS is based on the history and clinical manifestations (e.g., edema, proteinuria, hypoalbuminemia, and hypercholesterolemia in the absence of significant hematuria and hypertension).
- Massive proteinuria is reflected in urinary excretion of protein that often reaches levels in excess of 2 g/m² of body surface/day, with relatively greater clearance of low-molecular-weight proteins. Protein levels also form hyaline casts which are evident upon urinalysis.
- Oval fat bodies, as well as a few red blood cells (microscopic hematuria), can be found in most children.
- Specific gravity is high, proportionate to the amount of protein concentration.
- Glomerular filtration rate (urine output) is often normal if the child is well hydrated.
- Serology
- Total serum protein concentrations are reduced (albumin <2 g/dl) and plasma lipids are elevated (as high as 1500 mg/dL).
- Hemoconcentration results in a high platelet count. Hematocrit and hemoglobin may also be elevated.
- Serum sodium concentration is usually low due to edema (130 to 135 mEq/L).
- Total calcium levels are low but unreliable as calcium binds with albumin. Ionized calcium is a more reliable measure of calcium levels.
- Renal Biopsy is useful for providing information regarding the glomerular status and type of nephrotic syndrome, the likely response to drugs, and the probably course of the disease.
Therapeutic Management
The primary objective is to reduce the excretion of urinary protein and maintain protein-free urine. Additional objectives include prevention or treatment of acute infection, control of edema, establishment of good nutrition, and readjustment of any disturbed metabolic processes. Children with severe symptoms may be hospitalized for assessment and observation for evidence of infection, response to therapy, and parental education.
- General Measures are principally supportive. During the edema phase, the child is often limited to quiet activities. Infections are prevented/treated with antibiotics.
- Due to their susceptibility to pneumonia, the child should receive the pneumococcal conjugate vaccine (PCV13) and pneumococcal polysaccharide vaccine (PPSV23). However, these are not used while the child is on steroid therapy.
- Diet: the child in remission maintains a regular diet. However, salt is restricted during periods of massive edema and while on corticosteroid therapy. Water is seldom restricted.
- Protein replacement is logical, but there is no evidence that it is beneficial or alters the outcome of the disease. It may even be limited in the presence of azotemia and renal failure.
- Corticosteroid Therapy is the primary therapeutic agent in the management of MCNS, which is thought to have an immune-related cause. Prednisone (60 mg/m²/day, maximum 60 mg/day) is the steroid of choice. The drug is continued daily for 4 to 6 weeks then reduced to 40 mg/m², maximum 40 mg on alternate days for 2 to 5 months with taper. Studies show that the duration of steroid therapy for the initial episode should be at least 3 months.
- Children with MCNS typically relapse one to three times per year. Steroid-dependent children tend to have frequent relapses over many years and receive large amounts of steroids, which results in cushingoid features and may cause growth retardation. Steroid-resistant children are thought to have a high risk of developing chronic kidney disease.
Drug Alert: Steroids
Children who require frequent courses of steroid therapy are highly susceptible to complications of steroids, such as growth retardation, behavior changes, cataracts, increased appetite, obesity, hypertension, gastrointestinal bleeding, bone demineralization, infections, and hyperglycemia. Children who do not respond to steroid therapy, those who have frequent relapses, and those in whom the side effects threaten their growth and general health may be considered for a course of therapy using other immunosuppressant medications.
- Immunosuppressant Therapy: reduction of relapse rate and inducing long-term remission can be done with an oral alkylating agent, usually cyclophosphamide (Cytoxan) given orally for 12 weeks. Be aware of the potential side effects of immunosuppression, including neutropenia, infection, gonadal toxicity, malignancy, and hemorrhagic cystitis.
- Diuretics are sometimes useful when edema interferes with respiration or ambulation or there is hypertension or significant edema in the scrotum or labia. Infusion of salt-poor human albumin may be done to expand the plasma for prompt control, but frequent administration is required as the albumin is readily excreted.
Nursing Care Management
- Close monitoring: daily intake and output, progress of disease (urine albumin, daily weight, abdominal girth). Vital signs are also monitored to detect any early signs of complications such as shock or an infectious process.
- Assessment of edema: inspection and evaluation of degree of pitting and color and texture of the skin is part of nursing care. Elevation of edematous parts may be helpful, but diuresis with medications and salt and water restriction to remove edema fluid are the best therapies.
- Infection Precaution: these children are particularly vulnerable to upper respiratory tract infections. They should be protected from infected roommates, family, or visitors. Monitor vital signs to detect any early signs of an infectious process.
- Nutritional Support: edema of the intestinal mucosa causes anorexia, which is a difficult problem for children. A multidisciplinary approach is best for adequate, attractive diets. Small, frequent meals may be best tolerated. Salt and fluids are restricted during the edema phase.
- As the edema subsides, children are allowed increased fluids. Suitable recreational and diversional activities are also an important part of their care. Once the edema fluid has been lost, children can usually resume their normal activities without problems.
Home Care
Most children are treated at home during relapses unless the edema and proteinuria are severe. Teach parents to detect signs of relapse and to notify the health care provider if they occur.
- Parents should be taught in urine testing for albumin (daily during illness, twice a week during remission), administration of medications, and general care.
- Dietary restrictions in place during relapse and steroid therapy are not necessary for a child in remission.
- Infection precautions should remain in place. Parents should also be aware of the side effects of steroid therapy (e.g., rounding of the face, increased appetite, behavior changes, abdominal distention, and hirsutism). Reassure them that these will disappear gradually after discontinuation of the drug.