References:
- Psychiatric-Mental Health Nursing, 8th Edition, 978-1-975116-37-8, by Sheila L. Videbeck ([ebook] pp. 698-720)
- Lecturer (N/A)
Bipolar disorder (previously manic-depressive illness) involves extreme mood swings from episodes of mania to episodes of depression. This is one of the two primary mood disorders, with the other being major depressive disorder.
- During the manic phase, clients are euphoric, grandiose, energetic, and sleepless. They have poor judgment and rapid thoughts, actions, and speech. This typically lasts for about 1 week (unless the person is hospitalized and treated sooner), but it may be longer for some individuals.
- During depressed phases, mood, behavior, and thoughts are the same as in people diagnosed with major depression. This may even be the first phase that appears in a client with bipolar disorder, leading to a diagnosis of major depression until the person experiences a manic episode.
- Periods of euthymia—normal mood and affect—may be short-lived for some, while lasting for months or years for others.
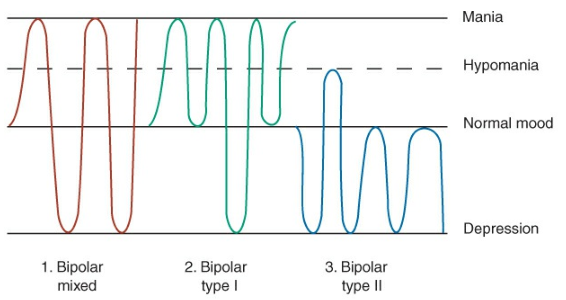
- The person with bipolar disorder cycles between depression and normal behavior (bipolar depressed) or mania and normal behavior (bipolar manic). A person with bipolar mixed episodes alternates between major depressive and manic episodes interspersed with periods of normal behavior. Each mood may last for weeks or months before the pattern begins to descend or ascend once again.
The Mood Disorder Questionnaire raises awareness for bipolar disorder.
Bipolar disorder occurs almost equally among men and women. It is more common in highly educated people. Because some people with bipolar illness deny their mania, prevalence rates may be higher than reported.
Bipolar disorder ranks second only to major depression as a cause of worldwide disability. The lifetime risk for bipolar disorder is at least 1.2% with a risk of completed suicide for 15%. Young men early in the course of the illness are at the highest risk for suicide, especially those with a history of suicide attempts or alcohol abuse as well as those recently discharged from the hospital.
Onset and Clinical Course
The first manic episode generally occurs in a person’s teens, 20s, or 30s. Currently, debate exists about whether or not some children diagnosed with attention-deficit/hyperactivity disorder actually have a very early onset of bipolar disorder.
Manic episodes typically begin with a rapid escalation of symptoms over a few days, and they last from a few weeks to several months. They tend to be briefer and end more suddenly than depressive episodes. Adolescents are more likely to have psychotic manifestations. The diagnosis of a manic episode or mania requires at least 1 week of unusual and incessantly heightened, grandiose, or agitated mood in addition to three or more of the following symptoms: exaggerated self-esteem, sleeplessness, pressured speech, flight of ideas, reduced ability to filter extraneous stimuli, distractibility, increased activities with increased energy, and multiple, grandiose, high-risk activities involving poor judgment and severe consequences, such as spending sprees, sex with strangers, and impulsive investments.
Clients often do not understand how their illness affects others. They may stop taking medications because they like the euphoria and feel burdened by the side effects, blood tests, and physicians’ visits needed to maintain treatment. Family members are concerns and exhausted by their loved ones’ behaviors; they often stay up late at night for fear that the manic person may do something impulsive and dangerous.
Psychodynamics
Bipolar disorder masks depression through episodes of mania.
- Biological: The most well-established neurochemical imbalance found in clients with bipolar disorder involves increased norepinephrine.
- Sociocultural:
- More cases of bipolar disorder is found in higher socioeconomic status.
Clinical Manifestations
Types of Bipolar Disorder
- Bipolar Type I: mania with at least one depressive episode. The severity of mania may result in hospitalization, psychotic features (hallucinations and delusions), impair functioning, and expose the client to risky behavior or legal issues.
- Bipolar Type II: recurrent depressive episodes with at least one hypomanic episode. A hypomanic episode is a period of abnormally and persistently elevated, expansive, or irritable mood lasting 4 days. It does not impair the ability to function and does not involve psychotic features.
- Bipolar Mixed: cycling between periods of mania, normal behavior, depression, normal behavior, mania, and so forth.
- Cyclothymic disorder is a separate diagnosis made for chronic mood swings that do not qualify for a diagnosis of bipolar disorder. While not as severe, mood swings are chronic and persistent.
| Category | Key Features |
|---|---|
| History | Difficult to obtain due to flight of ideas and distractibility. Requires multiple short sessions and input from family. |
| General Appearance and Behavior | Hyperactive, constantly moving, may wear flamboyant or sexually suggestive clothing that may also be inappropriate for the weather/situation. Exhibits pressured speech, rapid and loud, with frequent interruptions. |
| Mood and Affect | Euphoric, grandiose, labile mood. May also display irritability, sarcasm, or anger, especially when limits are set. |
| Thought Process and Content | Flight of ideas, circumstantial and tangential thinking. Impulsive, unrealistic goal setting, unable to complete tasks. May show grandiose delusions or psychotic features. |
| Sensorium and Intellectual Functioning | Often disoriented to time, poor attention and concentration, exaggerated claims of abilities, possible hallucinations if psychotic. |
| Judgment and Insight | Poor judgment, impulsive, lacks insight, believes nothing is wrong. Blames others for difficulties. |
| Self-Concept | Inflated self-esteem, unrealistic sense of self-worth, masks underlying chronic low self-esteem. |
| Roles and Relationships | Cannot fulfill responsibilities; hyper-social yet intrusive and confrontational. May engage in promiscuous or risky behavior. Relationships suffer due to unstable emotions and inability to delay gratification. |
DSM-V
(mn. MIGHT DIE)
- Motor agitation
- Ideas are racing in his thoughts
- Grandiosity; a delusion of grandeur
- Hours of sleep are decreased.
- Talkative, Flight of ideas,
- Distractibility
- Increase in goal-directed activity; competitiveness.
- Excessive involvement in activity such as gambling, pyramid schemes, and excessive sexual activity and potential paraphilic disorders.
Manic patients also engage in other criminal activities such as impulsive buying and kleptomania.
Medical Management
Treatment for bipolar disorder involves a lifetime regimen of medications—an antimanic agent called lithium or anticonvulsant medications used as mood stabilizers.
Lithium is a salt contained in the human body. 70% to 80% of clients in acute mania respond to lithium therapy. Lithium therapy decreases the range of bipolar behaviors and can also stabilize bipolar disorder by reducing the degree and frequency of cycling or eliminating manic episodes. Brand names of lithium preparations often include “lith” in the name as a prefix or suffix (e.g., Carbolith, Duralith, Eskalith, Lithotab, Lithane). The mechanism of action of lithium is unknown, but is thought to destroy catecholamines, inhibit neurotransmitter release, and decrease sensitivity of postsynaptic receptors.
- Lithium competes for salt receptor sites, and also affects calcium, potassium, magnesium, and glucose.
- Lithium’s action peaks in 30 minutes to 4 hours or regular forms and in 4 to 6 hours for slow-release forms. It crosses the blood-brain barrier and placenta and is distributed in sweat and breast milk. Lithium use during pregnancy is not recommended because it can lead to first-trimester developmental abnormalities.
- Onset of action is 5 to 14 days; with this lag period, antipsychotic or antidepressant agents are used carefully in combination with lithium to reduce symptoms in acutely manic or accurately depressed clients. The half-life of lithium is 20 to 27 hours.
Pharmacologic Considerations
- Prior to administering lithium, the nurse must first:
- Perform renal function tests (BUN, Crea.) as lithium is primarily excreted in the urine, and can be nephrotoxic.
- Perform serum lithium level measurements. A therapeutic level is 0.5 to 1.5 mEq/L, a maintenance level is 0.6 to 1.2 mEq/L, a toxic level is 2 mEq/L, and a lethal level is 3 mEq/L.
- During lithium therapy, increase fluid intake
- Tremors are an expected side effect, normally manifesting as fine tremors. It may become an early sign of toxicity when tremors become increasingly course.
- Lithium is tastes metallic. Inform the client that this is normal.
- Hold strenuous activities because sweating both decreases fluid and sodium loss, both of which can contribute to lithium toxicity.
- Increased “Uu”: diarrhea, polyuria, and vomiting.
- Mannitol is given for lithium toxicity to reverse the toxic effects by promoting diuresis of lithium. In extreme cases of lithium toxicity, dialysis is required.
Anticonvulsant drugs are used for the ~25% of people who do not respond to lithium therapy, or difficulty with side effects, drug interactions, or medical conditions (e.g., renal disease) that contraindicate the use of lithium. Several anticonvulsants traditionally used to treat seizure disorders have proved helpful in stabilizing the moods of people with bipolar illness. However, its mechanism of action is largely unknown; it is suspected that these drugs increase the brain’s threshold for dealing with stimuli.
- Carbamazepine (Tegretol), which has been used for grand mal and temporal lobe epilepsy as well as for trigeminal neuralgia, was the first anticonvulsant found to have mood-stabilizing properties, but the threat of agranulocytosis was of great concern.
- Serum drug levels need to be checked regularly for toxicity and therapeutic levels (4 to 12 mcg/mL).
- A white blood cell count is also performed regularly to monitor for suppression of white blood cells (agranulocytosis).
- Valproic acid (Depakote), also known as divalproex sodium or sodium valproate, is an anticonvulsant used for simple absence and mixed seizures, migraine prophylaxis, and mania. The mechanism of action is unclear.
- Therapeutic levels are monitored periodically to remain at 50 to 125 mcg/mL, as are baseline and ongoing liver function tests, including serum ammonia levels and platelet and bleeding times.
| Name | Side Effects | Nursing Implications |
|---|---|---|
| Carbamazepine (Tegretol) | Dizziness, hypotension, ataxia, sedation, blurred vision, leukopenia, and rashes | Rise slowly from sitting position (hypotension). Monitor gait and assist as necessary (ataxia). Report rashes to physician. |
| Divalproex (Depakote) | Ataxia, drowsiness, weakness, fatigue, menstrual changes, dyspepsia, nausea, vomiting, weight gain, and hair loss | Monitor gait as necessary (ataxia). Provide rest periods (fatigue). Administer with food (GI upset). Establish balanced nutrition (nausea and vomiting). |
| Gabapentin (Neurontin) | Dizziness, hypotension, ataxia, coordination, sedation, headache, fatigue, nystagmus, nausea, and vomiting. | Assist client in rise slowly from sitting position. Provide rest periods. Administer with food. |
Nursing Management
(mn. SEAL)
- Safety; at times, the nurse might need to follow the patient during their activities to maintain safety.
- Energy-rich food that can also be eaten
- Activities are normally solitary due to their disruptive and competitive nature. This includes journal writing, swimming, shadow boxing, and other outlets of motor agitation and restlessness such as fidget toys, Rubik’s cubes, etc.
- Lessen stimulation. This reduces reinforcements of the client’s manic state.
Nursing Diagnoses
- Risk for Injury related to impulsive behavior and aggression during manic episodes.
- Ineffective Coping related to difficulty managing mood swings and emotional regulation.
- Risk for Imbalanced Nutrition: Less Than Body Requirements related to decreased appetite during depressive episodes.
- Disturbed Sleep Pattern related to sleep disturbances during both manic and depressive phases.
The nurse manages common side effects of lithium therapy and prevents complications by counteracting their effects on body fluid and electrolyte balance and detecting toxicity.
| Effect | Nursing Intervention |
|---|---|
| Nephrotoxicity | Lithium is primarily excreted through the kidneys. It can accumulate in kidney cells and interfere with water reabsorption. Kidney function tests (e.g., serum creatinine, blood urea nitrogen) are important to monitor renal function. |
| Polyuria | The presence of lithium in the kidneys draws in more fluid from the body and inhibits water reabsorption, resulting in polyuria. This may contribute to dehydration. |
| Hand tremors | Evaluate for tremors, and differentiate it from other potential causes of tremors. The physician may alter the dosage if tremors affect functioning. Coarse tremors may also be a sign of lithium toxicity. |
| Diarrhea | Gastrointestinal side effects like diarrhea occur with lithium therapy. |
| Dry mouth | Lithium alters the concentration of fluids, leading to excessive urination and thirst, which produces dry mouth and dehydration. |
| Sodium imbalance | Because lithium is a salt, it displaces sodium in the body. The client becomes for susceptible to electrolyte imbalances. Dehydration associated with lithium therapy (polyuria, diarrhea) can also result in hemoconcentration hypernatremia. |
| Sweating | Sweating, especially for prolonged periods of time (e.g., during a marathon) can deplete body fluids and rapidly result in toxicity. |
(copied verbatim from Videbeck)
| Nursing Interventions | Rationale |
|---|---|
| Set and maintain limits on behavior that is destructive or adversely affects others. | Limits must be established by others when the client is unable to use internal controls effectively. The physical safety and emotional needs of other clients are important. |
| Initially, assign the client to the same staff members when possible, but keep in mind the stress of working with a client with manic behavior for extended periods of time. | Consistency can reassure the client. Working with this client may be difficult and tiring owing to his or her agitation, hyperactivity, and so forth. |
| Decrease environmental stimuli whenever possible. Respond to cues of increased agitation by removing stimuli and perhaps isolating the client; a private room may be beneficial. | The client’s ability to deal with stimuli is impaired. |
| Reorient the client to person, place, and time as indicated (call the client by name, tell the client your name, tell the client where he or she is, etc.) | Repeated presentation of reality is concrete reinforcement for the client. |
| Provide a consistent, structured environment. Let the client know what is expected of him or her. Set goals with the client as soon as possible. | Consistency and structure can reassure the client. The client must know what is expected before he or she can work toward meeting those expectations. |
| Spend time with the client. | Your physical presence is reality. |
| Show acceptance of the client as a person. | The client is acceptable as a person regardless of his or her behaviors, which may or may not be acceptable. |
| Use a firm yet calm, relaxed approach. | Your presence and manner will help communicate your interest, expectations, and limits, as well as your self-control. |
| Make only promises you can realistically keep. | Breaking a promise will result in the client’s mistrust and is detrimental to a therapeutic relationship. The client’s ability to respond to others and to deal with increased amounts and complexity of stimuli is impaired. |
| Limit the size and frequency of group activities based on the client’s level of tolerance. Help the client plan activities within his or her scope of achievement. | The client’s attention span is short, and his or her ability to deal with complex stimuli is impaired. |
| Avoid highly competitive activities. | Competitive situations can exacerbate the client’s hostile feelings or reinforce low self-esteem. |
| Evaluate the client’s tolerance for group activities, interactions with others, or visitors, and limit those accordingly. | The client is unable to provide limits and may be unaware of his or her impaired ability to deal with others. |
| Encourage the client’s appropriate expression of feelings regarding treatment or discharge plans. Support any realistic plan the client proposes. | Positive support can reinforce the client’s healthy expression of feelings, realistic plans, and responsible behavior after discharge. |