References:
- Brunner & Suddarth’s Textbook of Medical-Surgical Nursing, 15th Edition, ISBN 978-197-51-6103-3, by Janice L. Hinkle, Kerry H. Cheever, and Kristen J. Overbaugh (Ch. 19, [ebook] pp. 1530–1538)
Relevance
In my experience, atelectasis has exclusively been discussed as a product of other diseases and conditions.
Atelectasis refers to closure or collapse of alveoli and often is described in relation to chest x-ray findings and clinical signs and symptoms. It is one of the most commonly encountered abnormalities seen on a chest x-ray. Atelectasis may be acute or chronic and may cover a broad range of pathophysiologic changes, from microatelectasis (undetectable on an x-ray) to macroatelectasis with loss of segmental, lobar, or overall lung volume.
- The most commonly described is acute atelectasis, which occurs most often in the postoperative setting usually following thoracic and upper abdominal procedures or in people who are immobilized and have a shallow, monotonous breathing pattern.
- Excess secretions or mucus plugs may also cause obstruction of airflow and result in atelectasis in an area of the lung.
- Atelectasis also is observed in patients with chronic airway obstruction that impedes or blocks the flow of air to an area of the lung (e.g., obstructive atelectasis in the patient with lung cancer that is invading or compressing the airways). This type of atelectasis is more insidious and slower in onset.
Pathophysiology
Atelectasis may be described as either:
- Nonobstructive: atelectasis that results from reduced ventilation.
- Obstructive: atelectasis that results from any blockage that impedes the passage of air to and from the alveoli, reducing alveolar ventilation. This is the most common type and results from reabsorption of trapped gas, eventually draining the plugged lung fields of air and resulting in a collapse.
Causes may be due to a foreign body, tumor or growth in an airway, altered breathing patterns, retained secretions, pain, alterations in small airway function, prolonged supine positioning, increased abdominal pressure, reduced lung volumes due to musculoskeletal or neurologic disorders, restrictive defects, and specific surgical procedures (e.g., upper abdominal, thoracic, or open heart surgery).
- Postoperative patients are at high risk because of several factors: monotonous, low tidal breathing pattern may cause small airway closure and alveolar collapse. This can result from anesthesia or analgesia, supine positioning, splinting of the chest wall because of pain, or abdominal distention. Additionally, secretion retention, airway obstruction, and an impaired cough reflex (or reluctance due to pain) may also occur.
- Impaired cough mechanisms can also result in atelectasis from bronchial obstruction by secretions, such as in patients with musculoskeletal or neurologic disorders, and those who are debilitated and confined to bed.
- Excessive pressure on the lung tissue can also result in atelectasis (i.e., compressive atelectasis) as lung expansion on inspiration is restricted. Such pressures can be produced by pleural effusion, pneumothorax, hemothorax, pericardial effusion, tumor growth within the thorax, or an elevated diaphragm.
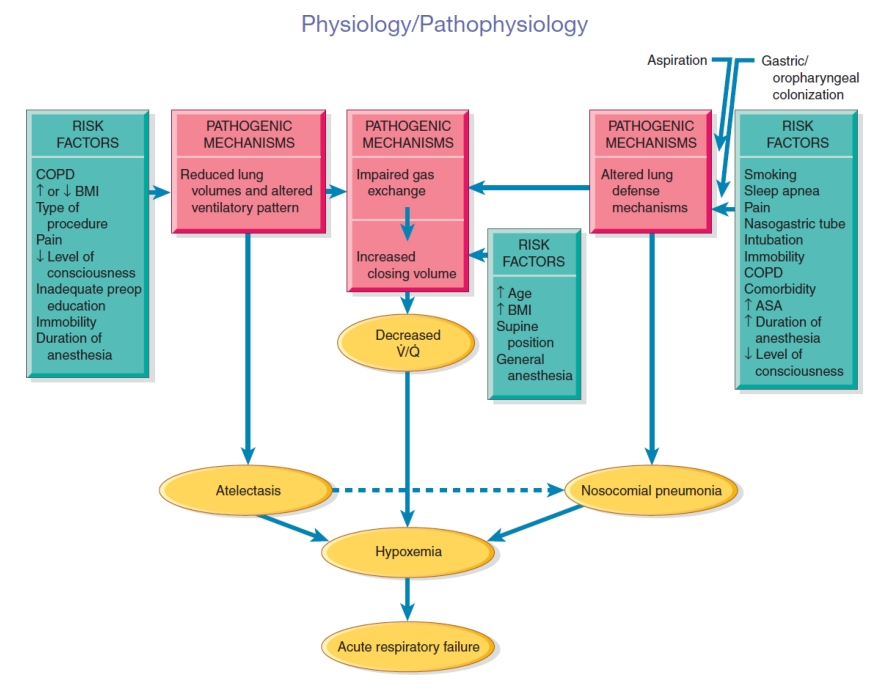
(Brunner & Suddarth) Relationship of risk factors, pathogenic mechanisms, and consequences of acute atelectasis in the postoperative patient:
Clinical Manifestations
The development of atelectasis usually is insidious.
- Signs and symptoms include increasing dyspnea (shortness of breath), cough, and sputum production.
- In acute atelectasis involving a large amount of lung tissue (lobar atelectasis), marked respiratory distress may be observed. In addition to the previously mentioned signs and symptoms, tachycardia, tachypnea, pleural pain, and central cyanosis (late sign of hypoxemia) may be anticipated. Patients characteristically have difficulty breathing in the supine position and are anxious.
- In chronic atelectasis, signs and symptoms are similar to those of acute atelectasis. However, the chronic nature of the alveolar collapse predisposes patients to infection distal to the obstruction. Therefore, the signs and symptoms of a pulmonary infection may also be present.
Assessment and Diagnostic Findings
Clinically significant atelectasis is generally characterized by increased work of breathing and hypoxemia (i.e., a decrease in oxygen tension in the arterial blood).
- Decreased breath sounds and crackles are heard over the affected area.
- A chest x-ray may suggest a diagnosis of atelectasis before clinical symptoms appear; the x-ray may reveal patchy infiltrates or consolidated areas.
- Depending on the degree of hypoxemia, pulse oximetry (SpO₂) may demonstrate a low saturation of hemoglobin with oxygen (<90%) or a lower-than-normal partial pressure of arterial oxygen (PaO₂, normally >80%)
Severity
Tachypnea, dyspnea, and mild-to-moderate hypoxemia are hallmarks of the severity of atelectasis.
Prevention
- Frequent turning and repositioning, especially from supine to upright, promotes ventilation and prevents secretions from accumulating.
- Encourage early mobilization from bed to chair followed by early ambulation.
- Voluntary deep-breathing maneuvers and coughing at least every two hours assist in preventing and treating atelectasis. The performance of these maneuvers requires the patient to be alert and cooperative. Patient education and reinforcement are key elements to the success of these interventions. The use of incentive spirometry or voluntary deep breathing enhances lung expansion, decreases the potential for airway closure, and may generate a cough.
- Administer prescribed opioids and sedatives judiciously to prevent respiratory depression.
- Perform postural drainage and chest percussion, if indicated.
- Institute suctioning to remove tracheobronchial secretions, if indicated.
Incentive Spirometry
Incentive spirometry is a method of deep breathing that provides visual feedback to encourage the patient to inhale slowly and deeply to maximize lung inflation and prevent or reduce atelectasis. It ensures that the volume of air inhaled increases gradually as the patient takes deeper and deeper breaths. There are two types:
In Volume-type Incentive Spirometry, the tidal volume is set using the manufacturer’s instructions. The patient takes a deep breath through the mouthpiece, pauses at peak lung inflation, and then relaxes and exhales. Taking several normal breaths before attempting another with the incentive spirometer helps avoid fatigue. The volume is periodically increased as tolerated.
In Flow-type Incentive Spirometry, there is no preset volume—the spirometer contains a number of movable balls that are pushed up by the force of the breath and held suspended in the air while the patient inhales. The amount of air inhaled and the flow of the air are estimated by how long and how high the balls are suspended.
The inspired air helps inflate the lungs. (If flow-type,) The ball or weight in the spirometer rises in response to the intensity of the intake of air. The higher the ball rises, the deeper the breath. The nurse provides the following instructions:
- Assume a semi-Fowler position or an upright position before initiating therapy.
- Use diaphragmatic breathing.
- Place the mouthpiece of the spirometer firmly in the mouth, breathe are in slowly through the mouth, and hold the breath at the end of inspiration for about 3 seconds to maintain the ball/indicator between the lines. Exhale slowly through the mouthpiece.
- Cough during and after each session. If postoperative, splint incisions when coughing.
- Perform the procedure approximately 10 times in succession, repeating the 10 breaths with the spirometer each hour during waking hours.
Management
The goal of the treatment is to improve ventilation and remove secretions. Strategies to prevent atelectasis, which include frequent turning, early ambulation, lung volume expansion maneuvers (e.g., deep-breathing exercises and incentive spirometry), and coughing, also serve as the first-line measures to minimize or treat atelectasis by improving ventilation.
In patients who do not respond to first-line measures or who cannot perform deep-breathing exercises, other treatments such as positive end-expiratory pressure, continuous positive airway breathing, or bronchoscopy may be used. Importantly, before initiating more complex, costly, and labor-intensive therapies, the nurse must always consider:
- “Has the patient been given an adequate trial of deep-breathing exercises?”
- “Has the patient received adequate education, supervision, and coaching to carry out the deep-breathing exercises?”
- “Have other factors been evaluated that may impair ventilation or prevent a good patient effort (e.g., lack of turning, mobilization, excessive pain, excessive sedation)?”
Etiologic Basis for Management
- Bronchial obstruction from secretions: removal of secretions by coughing or suctioning, chest physiotherapy, postural drainage, small-volume nebulization of expectorants, and bronchoscopy.
- Bronchoscopy is used if all previous methods fail. It is an excellent measure to acutely remove secretions and increase ventilation, but poses further risk once removed; the nurse must assist the patient with maintaining the patency of airways after bronchoscopy, using the traditional techniques of deep breathing, coughing, and suctioning. Otherwise, severe or massive atelectasis may lead to acute respiratory failure. Endotracheal (ET) intubation and mechanical ventilation may be necessary.
- Compression of lung tissue (compressive atelectasis): decrease compressive forces. In the case of pleural effusion, management is thoracentesis or chest tube insertion. Previous methods of improving lung expansion still apply.
- Chronic atelectasis due to obstruction focuses on removing the cause of obstruction. Bronchoscopy, cryotherapy, or laser therapy may remove obstructions from lung cancer or a nonmalignant lesion. Obstructions caused by lung cancer can be managed via the placement of an airway stent or radiation therapy.
- Long-term collapse may make reopening and reaerating improbable. Surgical management may be indicated.