References:
- Brunner & Suddarth’s Textbook of Medical-Surgical Nursing, 15th Edition, ISBN 978-197-51-6103-3, by Janice L. Hinkle, Kerry H. Cheever, and Kristen J. Overbaugh (Ch. 23)
There are various methods to reperfuse ischemic myocardial tissue for use when conservative management methods do not take effect in patients. These includes Percutaneous Coronary Interventions (PCIs) and Coronary Artery Bypass Grafting (CABG) surgery.
Percutaneous Coronary Interventions
Invasive interventional procedures to treat CAD include PTCA and intracoronary stent implantation. These procedures as classified as percutaneous coronary interventions as they are performed through a skin puncture rather than a surgical incision.
- Percutaneous Transluminal Coronary Angioplasty (PTCA): a balloon-tipped catheter is used to open blocked coronary vessels and resolve ischemia. It is used in patients with angina and as an intervention for ACS. Catheter-based interventions can also be used to open blocked CABGs (discussed later). The purpose of a PTCA is to improve blood flow within a coronary artery by compressing the atheroma. The procedure is attempted when the interventional cardiologist determines that PTCA can improve blood flow to the myocardium.
- Sheaths, a hollow catheter, is inserted usually in the femoral artery (and sometimes the radial artery). This serves as a conduit for other catheters, which pass through the femoral or radial artery, through the aorta, and into the coronary arteries.
- Angiography is performed with injected radiopaque contrast agents (“dye”) to identify the location and extent of the blockage.
- A balloon-tipped dilation catheter is passed through the sheath and positioned over the lesion. The physician determines the catheter position by examining markers on the balloon that can be seen with fluoroscopy. After proper positioning, the balloon is inflated with high pressure for several seconds then deflated.
- This pressure compresses and often “cracks” the atheroma, and also stretches the media and adventitia of the coronary artery. Inflations may be repeated with different balloon sizes until the goal is reached (usually defined as a residual stenosis of less than 10% and improved blood flow). Other benchmarks for success in treatment is the arterial lumen and clinically no obvious arterial trauma.
- A stent may be placed in the intima of the vessel to maintain patency of the artery after the balloon is withdrawn.
- Coronary Artery Stent: after PTCA, the treated area may close off partially or completely— restenosis. Vasoconstriction, clotting, and scar formation may occur as an acute inflammatory response. To overcome these risks, a stent may be placed. It is a metal mesh that provides structural support to a vessel at risk of acute closure. The stent is initially positioned over the angioplasty balloon. When the balloon is inflated, the mesh expands and presses against the vessel wall, holding the artery open. This is left permanently in place, at some point becoming covered in new endothelium making it a part of the vessel wall.
- Bare metal stents only serve as stents. They do are not coated in medications.
- Drug-eluting stents (DES) are those covered with medications, such as sirolimus or paclitaxel, which may minimize the formation of thrombi or scar tissue within the coronary artery lesion.
- Due to the risk of thrombus formation, the patient with a stent is placed on anticoagulant therapy— a lifetime of Aspirin and one year of clopidogrel following stent placement.
Complications of PCI
The pressure placed on the coronary artery can result in coronary artery dissection, perforation, abrupt closure, or vasospasm. Acute MI, serious arrhythmias (e.g., ventricular tachycardia), and cardiac arrest can occur, at times requiring emergency surgical treatment.
The site of insertion can also experience complications: bleeding at the insertion site, retroperitoneal bleeding, hematoma, and arterial occlusion. There is also a risk of acute kidney injury from the contrast agent used during the procedure.
Postprocedure care is similar to a diagnostic cardiac catheterization. Patients who are not already hospitalized are admitted the day of the PCI. If no complications arise, they may return home in the same day. If the procedure was emergent, the patient may stay in the critical care unit for a few days.
- During the procedure, patients are given IV heparin or a thrombin inhibitor, requiring close monitoring for signs of bleeding.
- Hemostasis after sheath removal can be achieved through vascular closure devices (e.g., Angio-Seal, VasoSeal), suturing, direct manual pressure, a mechanical compression device, or a pneumatic compression device.
- Patients may return to the nursing unit with the large peripheral vascular access sheaths in place, only removed once blood studies indicate that heparin is no longer active and the clotting time is within acceptable range (often within a few hours). During this period, the patient remains flat on bed and keeps the affected leg straight until the sheaths are removed and then for a few hours afterwards to maintain hemostasis.
- Immobility and bed rest may cause discomfort, potential indicators for analgesics and sedation. Repositioning and heat application for back pain may also be used as nonpharmacologic interventions.
- The removal of a sheath may stimulate the vasovagal response, slowing the heart rate. A dose of IV Atropine is usually given to treat this response.
- A pressure dressing is applied after hemostasis. Ambulation may begin within hours depending on the case. The patient is taught to identify and report signs of bleeding and hematoma.
Coronary Artery Revascularization
The most common CABG techniques have been performed for more than 40 years, and continue to improve. Coronary artery bypass graft (CABG) is a surgical procedure in which a blood vessel is grafted to an occluded coronary artery so that blood can flow beyond the occlusion; it is also called a bypass graft. These are used in patients where:
- Angina cannot be controlled with medication or PCI.
- The coronary artery involved is the left main coronary artery or the CAD spans multiple vessels.
- MI, arrhythmias, or heart failure is likely.
- PCI has been unsuccessful.
Additional requirements for consideration of CABG include at least a 70% occlusion in any vessel or a 50% occlusion in the left main coronary artery. Without this threshold, the addition of a graft is unlikely to improve the patient’s condition.
Traditional Coronary Artery Bypass Graft
Blood Vessels for Use
The arteries to be used in current CABG guidelines are the internal thoracic (mammary) arteries. Their histologic characteristics make them less likely to lose patency (vasoactive molecules; anti-inflammatory cytokines). This results in greater survival and a greater than 90% patency after 20 years— it is the first conduit to be considered.
Arterial grafts are also used over venous grafts because they do not develop atherosclerotic changes as quickly and remain patent for longer. However, they may be used if the internal thoracic arteries are not long enough for multiple bypasses. A combination may be used for such cases. The vein of choice is the greater saphenous vein, followed by the lesser saphenous vein. These are removed from the leg and grafted to the ascending aorta and to the coronary artery distal to the lesion. These veins often become atherosclerotic within 5 to 10 years.
Traditionally, general anesthesia is used for a median sternotomy and a cardiopulmonary bypass (CPB) machine. Once connected, the blood vessel to be used is grafted distal to the coronary artery lesion, bypassing the obstruction. CPB is discontinued once patency is established, chest tubes and epicardial pacing wires are placed, and the incision is closed. Monitoring continues in the critical care unit.
Cardiopulmonary Bypass (CPB)
Also known as extracorporeal circulation, this procedure allows for mechanical circulation and oxygenation of blood for the body while bypassing the heart and lungs. CPB maintains perfusion to body organs and tissues and allows the surgeon to complete the anastomoses in a motionless, bloodless surgical field.
- A cannula is placed in the right atrium, vena cava, or femoral vein to withdraw blood from the body (suction).
- The cannula is connected to tubing filled with an isotonic crystalloid solution, then filtered, oxygenated, cooled, or warmed by the machine, and then returned to the body through a cannula inserted in the ascending aorta (or femoral artery).
- The heart is stopped through injection of a potassium-rich cardioplegia solution into the coronary arteries.
- The patient receives heparin to prevent clotting and thrombus formation in the bypass circuit when blood comes in contact with the surfaces of the tubing. Protamine sulfate is given to reverse the effects of heparin after disconnection from the CPB machine.
Alternative Coronary Artery Bypass Graft
An off-pump coronary artery bypass (OPCAB) has been used successfully in many patients. It involves a standard medial sternotomy incision, but the surgery is performed without CPB. A beta-adrenergic blocker and myocardial stabilization device are used to keep the heart still enough for surgery while beating.
- Short-term postoperative morbidity and complication is suggested to be lower with OPCAB.
- However, long-term mortality is lower and graft patency rate is higher in on-pump CABG.
The need for a median sternotomy has also been eliminated with the use of minimally invasive surgical techniques. These are endoscopic techniques that use a right or left thoracotomy approach and a robotic system to place bypass grafts, with the patient potentially not requiring CPB. This is most commonly used in patients with left anterior descending artery occlusions, and can be used for select patients that do not require bypass grafts to several vessels. Minimal invasiveness results in faster recovery, less required blood transfusions, fewer respiratory complications, and a lower likelihood of experiencing acute kidney injury.
Complications of both CABG types
Hemorrhage, arrhythmias, and MI can occur. The patient may require interventions for more than one complication at a time. A multidisciplinary approach is necessary to achieve the desired patient outcomes.
CABG is not a cure for CAD. Angina, exercise intolerance, and other symptoms experienced before CABG may recur. Medications used by the patient before surgery may continue to be necessary. Lifestyle modifications remain important for the continued viability of the newly implanted grafts.
Nursing Management
Cardiac surgery patients have many of the same needs and require the same perioperative care as other surgical patients, along with some special needs.
Preoperative Management
A comprehensive pre-operative medical management prevents complications and improves outcomes. Patients who are due for CABG surgeries tend to be older and have multiple comorbidities. The use of aspirin, beta-blockers, and statins during the preoperative period is associated with better outcomes.
- Preoperative use of aspirin is associated with a reduction in perioperative morbidity and mortality.
- Beta-blockers, when given at least 24 hours before CABG, reduce the incidence of postoperative atrial fibrillation.
- Statins have been shown to reduce the rates of postoperative MI, atrial fibrillation, neurologic dysfunction, renal dysfunction, infection, and death.
Assessing the Patient is often done on the day of the procedure, when the patient is admitted. A thorough history and physical examination is done. Testing includes a chest x-ray; ECG; laboratory tests (coagulation studies); and blood typing and cross-matching. The nurse identifies disorders that could complicate or affect the postoperative course, such as diabetes, hypertension, and lung disease.
- Baseline data is obtained for physiologic, psychological, and social status. Of particular importance are the patient’s usual functional level, coping mechanisms, and available support systems.
- Cognitive status is checked for considerations of greater assistance and subacute care prior to returning home. Older adults are at greater risk for suffering adverse cognitive outcomes following cardiac surgery.
- Cardiovascular status is determined by reviewing the patient’s symptoms, including past and present experiences with chest pain, palpitations, dyspnea, intermitted claudication (leg pain that occurs with walking), and peripheral edema.
- Other medical information such as history of major illnesses; previous surgeries; medication; and the use of illicit and over-the-counter drugs, herbal supplements, alcohol, and tobacco is also obtained.
- If diabetes is present, determine blood glucose control— poor control results in higher incidence of postoperative complications.
- Psychosocial assessment and learning needs assessment are important. Great stress to both the family and the patient can bring about poorer patient outcomes. Some anxiety is good; worrying can help patients identify priorities and coping strategies that help them face the threat of surgery. The nurse can provide information about the procedure, postoperative course, recovery, fears, future health status, coping mechanisms, and support systems available during and following hospitalization.
- This information is important for comparison to post-operative status.
Reducing Fear and Anxiety is imperative. The patient and family are given ample time to express their fears and concerns of pain, of changes in body image, of the unknown, of disability, or even of death.
- The nurse can help alleviate these concerns with the provision of information, such as a description of the sensations that patient can expect, including the preoperative sedation, surgical anesthesia, and postoperative pain management.
- The nurse reassures the patient that fear of pain is normal, and while some pain will be experienced, medications for relieving pain is also provided, and that the patient will be closely monitored. This is a good time for educating the patient for when to request pain medications— before the pain becomes severe.
- Concerns of changes in body image (scarring) are discussed with the patient. Any misconceptions are cleared up.
- The fear of the patient dying is also explored and normal. Further exploration of their feelings about the prospect may be discussed.
- Extreme anxiety or fear and for whom emotional support and education are not successful, antianxiety medication such as lorazepam may be helpful.
Complications can begin to arise even in the preoperative phase. Angina may occur because of increased stress and anxiety related to the forthcoming surgery. Typical therapy for this pain is often successful (nitroglycerin), though some may require oxygen and IV nitroglycerin infusions. If the patient is physiologically unstable, preoperative management may take place in a critical care unit.
Patient Education is provided with information on:
- How the patient should take or stop specific medications, including anticoagulant agents, antihypertensive medications, and medications that control diabetes.
- Showering with an antiseptic solution (e.g., chlorhexidine gluconate) and applying mupirocin calcium 2% ointment to each nostril to help reduce the risk of surgical site infections. This has been found to be effective because cardiac surgical infections are often caused by Staphylococcus aureus, which are commonly found in the nasal passages.
- Information about hospitalization and surgery should also be provided. Details about the equipment, tubes, and lines that will be present after surgery and their purposes are explained to the purpose to help reassure the patient.
- Postoperative care and procedures are taught and practiced with the patient and family. This includes deep breathing and coughing, incentive spirometry, and foot exercises.
Intraoperative Management
The perioperative nurse performs assessments and prepares the patient. In addition to assisting with the surgical procedure, perioperative nurses are responsible for the comfort and safety of the patient. Possible intraoperative complications include low cardiac output, arrhythmias, hemorrhage, MI, organ failure from shock, and thromboembolic events including stroke.
Astute intraoperative nursing assessment is critical to prevent, detect, and initiate prompt intervention for these complications. Before the chest incision is closed, chest tubes are inserted to evacuate air and drainage from the mediastinum and the thorax. Temporary epicardial pacemakers may be used in the event of persistent bradycardia perioperatively.
Postoperative Management
Initial postoperative care focuses on achieving or maintaining hemodynamic stability and recovery from general anesthesia. Care may be provided in the post-anesthesia care unit (PACU) or ICU. The immediate postoperative period for the patient who has undergone cardiac surgery presents many challenges to the health care team. All efforts are made to facilitate the transition from the operating room to the ICU or PACU with minimal risk. Specific information about the surgical procedure and important factors about postoperative management are communicated by the surgical team and anesthesia personnel to the critical care or PACU nurse, who then assumes responsibility for the patient’s care. After the patient’s cardiac status and respiratory status are stable, the patient is transferred to a surgical progressive care unit with telemetry. Care in both the ICU and progressive care unit focuses on monitoring of cardiopulmonary status, pain management, wound care, progressive activity, and nutrition. Education about medications and risk factor modification is emphasized.
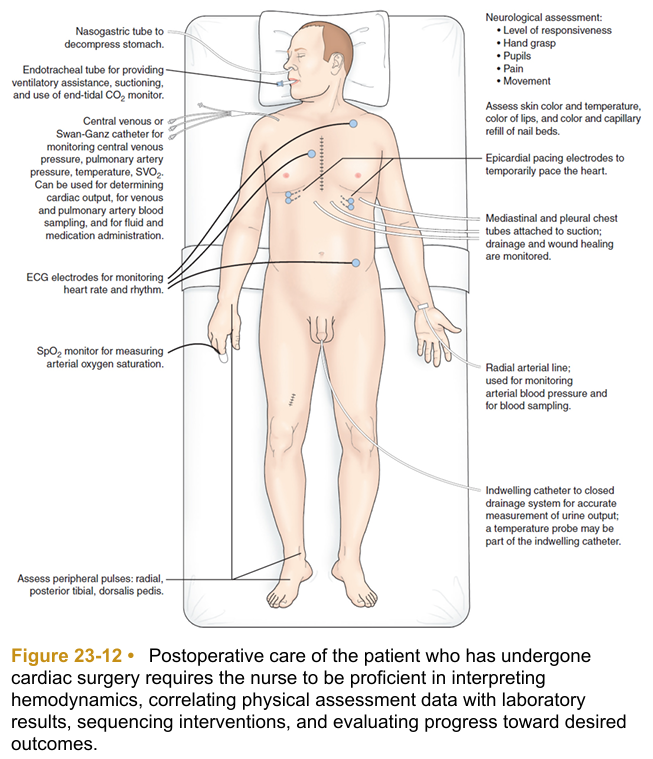
When the patient is admitted to the critical care unit or PACU, nursing and medical personnel perform a complete assessment of all systems at least every 4 hours. It is necessary to assess the following parameters:
- Neurologic status: level of responsiveness, pupil size and reaction to light, facial symmetry, movement of the extremities, and hand grip strength
- Cardiac status: heart rate and rhythm, heart sounds, pacemaker status, arterial blood pressure, and central venous pressure (CVP). A pulmonary artery catheter is may be used to monitor other hemodynamic parameters in select patients.
- Cardiac status: chest movement, breath sounds, ventilator settings, respiratory rate, peak inspiratory pressure, percutaneous oxygen saturation (SpO2), end-tidal carbon dioxide (CO2), pleural chest tube drainage, arterial blood gases.
- Peripheral vascular status: peripheral pulses; color of skin, nail beds, mucosa, lips, and earlobes; skin temperature; edema; condition of dressings and invasive lines Renal function: urinary output; serum creatinine and electrolytes.
- Fluid and electrolyte status: strict intake and output, including all IV fluids and blood products, output from all drainage tubes; clinical and laboratory indicators of imbalance
- Pain: nature, type, location, and duration; apprehension; response to analgesics
- Psychological and emotional status can also be checked once the patient regains consciousness and progresses through the postoperative period. The nurse should check for denial, depression, or postoperative delirium.
- Contraptions: all equipment and tubes should be assessed for proper functioning.
Nursing Diagnoses After Cardiac Surgery
- Impaired cardiac output associated with blood loss and compromised myocardial function
- Impaired gas exchange associated with chest surgery
- Risk for hypovolaemia or hypervolaemia and electrolyte imbalance associated with alterations in blood volume
- Risk for acute confusion associated with alteration in sleep–wake cycle, impaired metabolic functioning, use of multiple medications
- Acute pain associated with surgical trauma and pleural irritation caused by chest tubes
- Risk for impaired cardiac function associated with alterations in afterload that may compromise renal perfusion
- Impaired thermoregulation associated with infection or postpericardiotomy syndrome
- Lack of knowledge about self-care activities
The patient is also continuously assessed for impending complications. Prevention, early identification, and intervention is a multidisciplinary effort.
- Decreased cardiac output
- Fluid volume and electrolyte imbalance
- Impaired gas exchange
- Impaired cerebral circulation
| Nursing Goal | Assessment Cues | Interventions |
|---|---|---|
| Maintaining Cardiac Output | Continuous monitoring—urine output reflects cardiac function. Urine output less than 0.5 mL/kg/h may indicate a decrease in cardiac output or inadequate fluid volume. Body tissues are inspected for cyanosis or duskiness. Distention of the neck veins while the head of the bed is 30 degrees or more may signal right-sided heart failure. | Report any indications of decreased cardiac output promptly. When indicated, blood components; fluids; and antiarrhythmics, diuretics, vasodilators, or vasopressors are prescribed. |
| Promoting Adequate Gas Exchange | Patency and placement of the endotracheal tube is assessed regularly. ABG values are compared with baseline data, and changes are reported promptly. | Suctioning is necessary when crackles or coughing is present. When hemodynamically stable, body positions can be changed every 1 to 2 hours. Frequent changes provide for optimal pulmonary ventilation and perfusion, allowing the lungs to expand more fully. Weaning is utilizes for the removal of the endotracheal tube. After extubation, deep breathing and coughing is done at least every 1 to 2 hours. |
| Maintaining Fluid and Electrolyte Balance | Carefully assess intake and output. Record all sources of gain or less, including IV, nasogastric tube, oral fluids, urine, nasogastric drainage, and chest drainage. Correlate hemodynamic parameters with intake, output, and weight to determine the adequacy of hydration and cardiac output. Monitor serum electrolytes. | Report any indications of dehydration, fluid overload, or electrolyte imbalance promptly. |
| Minimizing Confusion | Assess for postoperative delirium: restlessness, agitation, visual and auditory hallucinations, and paranoia. | At times, correcting physiologic problems such as metabolic and electrolyte imbalances can help. Behavioral interventions (e.g., frequent reorientation) may be used. |
| Relieving Pain | Assess for verbal and nonverbal indicators of pain. Pain is most intense when coughing, turning, and moving. *Assess for signs of adverse effects of opioids. | Record the nature, type, location, and duration of pain. Encourage the client to accept pain medication on a regular basis, and adjunctive pain relievers (anti-inflammatory agents, muscle relaxants). Support the incision with a folded bath blanket or small pillow during deep breathing and coughing to minimize pain. |
| Maintaining Adequate Tissue Perfusion | Regularly palpate peripheral pulses to assess for arterial obstruction. If any pulse is absent, it may be due to prior catheterization, chronic peripheral vascular disease, or a thromboembolic obstruction. Assess for acute onset of chest pain or respiratory distress (pulmonary embolus, M.I.) Assess for abdominal or back pain (mesenteric emboli) Assess for pain, cessation of pulses, blanching, numbness, or coldness in an extremity Assess for one-sided weakness and pupillary changes (stroke) Assess urine output and renal function. | Immediately report newly identified absence of any pulse. Apply sequential pneumatic compression devices as prescribed. Discourage crossing of legs Avoid elevating knees on the bed. Omit pillows in the popliteal space. Begin passive exercises followed by active exercises to promote circulation and prevent venous stasis. |
| Maintaining Normal Body Temperature | Assess for hypothermia. This is often normal from induced hypothermia, but core temperature should be reached postoperatively. | Heated air blanket systems Antipyretics Care of infection-prone sites (e.g., catheters, tube insertions, incisions) to prevent infection. Clearance of pulmonary secretions with frequent repositioning of the patient, suctioning, and chest physical therapy, as well as educating and encouraging the patient to breathe deeply and cough. Discontinue tubes and lines as early as possible to avoid infection. |