References:
- Brunner & Suddarth’s Textbook of Medical-Surgical Nursing, 15th Edition, ISBN 978-197-51-6103-3, by Janice L. Hinkle, Kerry H. Cheever, and Kristen J. Overbaugh (Ch. 57, [ebook] pp. 4935–5022)
- Saunders Comprehensive Review for the NCLEX-RN Examination, 9th Edition, ISBN 978-032-37-9530-2, by Linda Anne Silvestri, Angela E. Silvestri, and Jessica Grimm (Ch. 70, pp. 1046–1053), not yet fully adapted
- Comprehensive Nursing Licensure Review Book: Local and International Test Prep, Volumes 1 and 2, ISBN 978-971-51-3383-8, by Josie Quiambao-Udan
- The Topranker’s Guide: A Comprehensive Study Guide for the Nurse Licensure Exam
- Lecturer (Coprade)
This page is huge!
If you’re reading this to study for the board exam, it might be better to read the review edition of this note instead. It’s a summary of this topic with information limited to those that appear pertinent for the licensure exam. This page is as thorough as it is because it’ll be my reference in case I ever get assigned to a Burn Unit in the future.
The main body of the discussion is based on Brunner & Suddarth, with some extra information sprinkled in from other sources. I’ve indicated the respective sources for additional information.
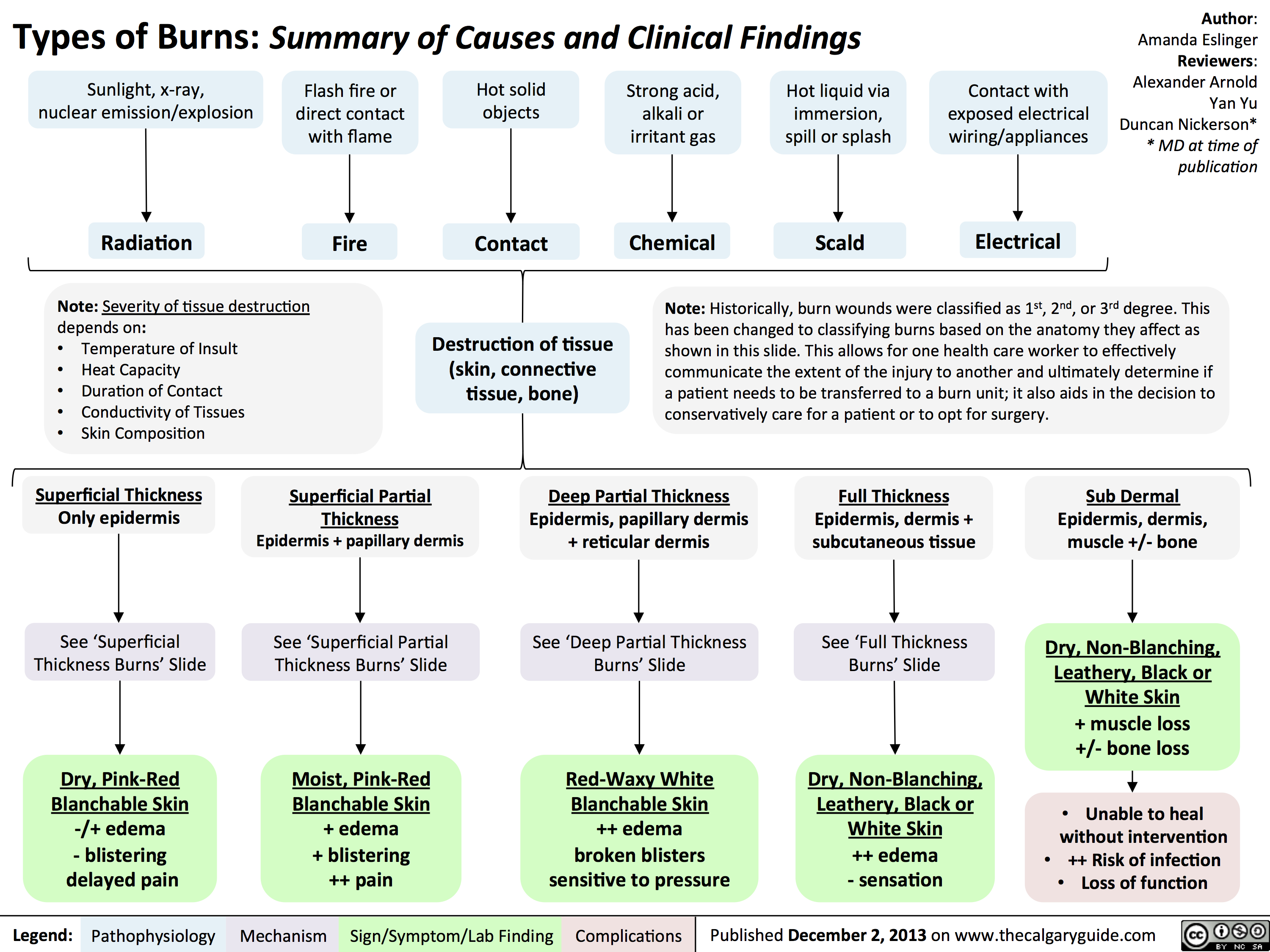
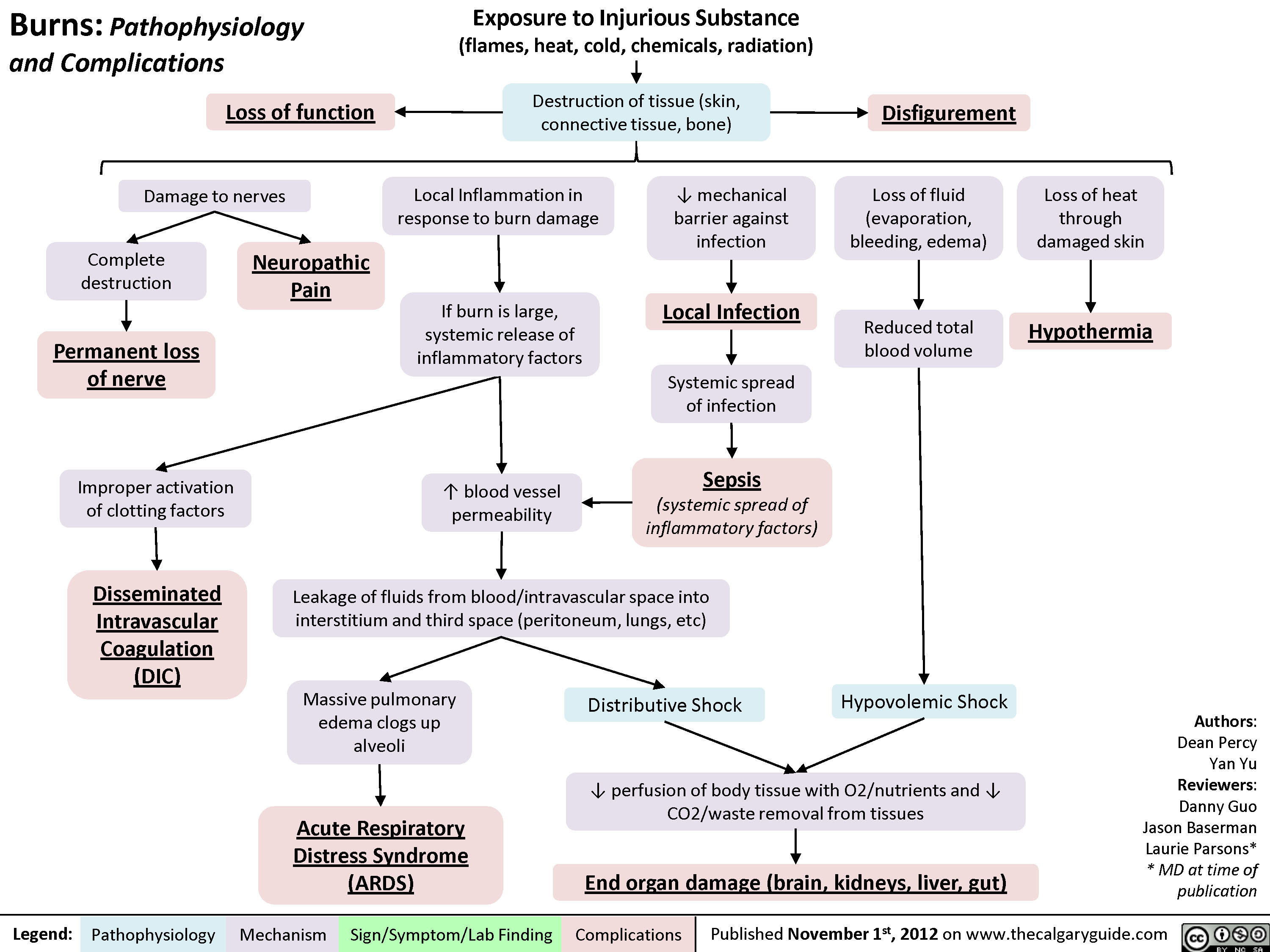
A burn is an injury to the skin or other organic tissue primarily caused by thermal, radioactive, electrical, or chemical exposure. This poses many problems as destruction of tissue and cells results in impaired skin integrity, fluid imbalance, and electrolyte imbalance.
- Thermal Burns: exposure to high temperatures, the most common form of burning. The most common cause is fire, which requires four elements to appear:
- Heat: sufficient heat is required for a heat to sustain its chain reaction.
- Oxygen: oxygen is essential for the chemical reaction of a fire. Oxygen is a flammable gas.
- Fuel: fuel is continuously consumed in fire
- Chain Reaction/Combustion
- Chemical Burns: exposure to highly acidic or highly alkaline substances.
- Electrical Burns: exposure to electricity, the most lethal form of burning.
- Radiation Burns: exposure to UV or gamma radiation.
Severity
Factors Affecting Burn Severity
Age of the patient; depth of the burn; amount of surface area of the body burned; the presence of inhalation injury; presence of other injuries; location of the injury in areas such as the face, the perineum, hands, or feet; and the presence of comorbid conditions.
- Surface area and age: In adults, a %TBSA of ≥20%–25% may be considered a large or extensive burn. In children, a large or extensive burn is ≥10%. (Saunders)
- Burn location: (Saunders)
- Burns of the head, neck, and chest are associated with pulmonary complications.
- Burns of the face are associated with corneal abrasion.
- Burns of the ear are associated with auricular chondritis.
- Burns of the hands and joints require intensive therapy to prevent disability.
- Burns of the perineal area is prone to autocontamination by urine and feces.
- Circumferential burns of the extremities can produce a tourniquet-like effect and lead to vascular compromise (compartment syndrome).
- Circumferential thorax burns leads to inadequate chest wall expansion and pulmonary insufficiency.
A burn can be classified according to the depth of tissue involved:
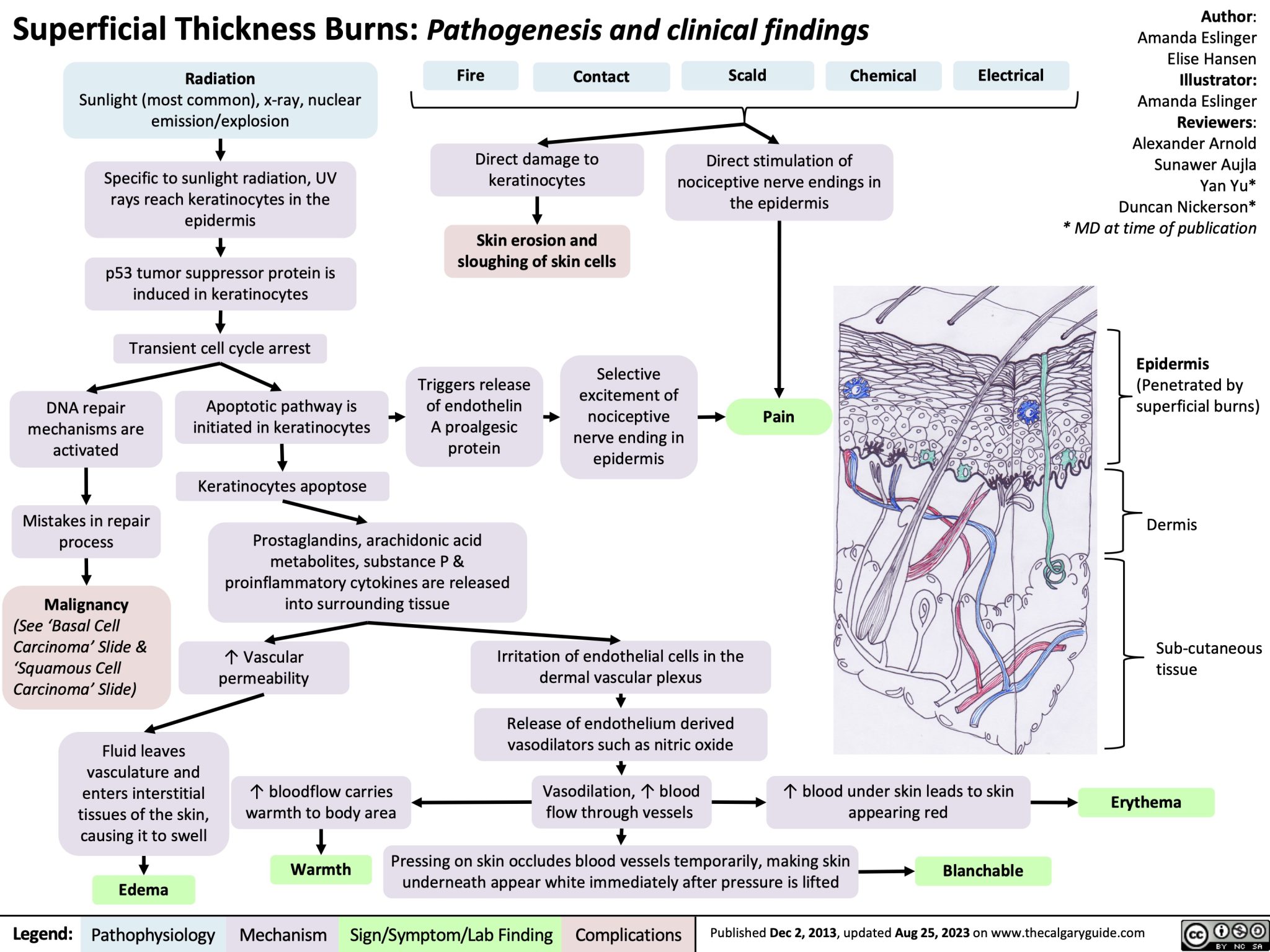
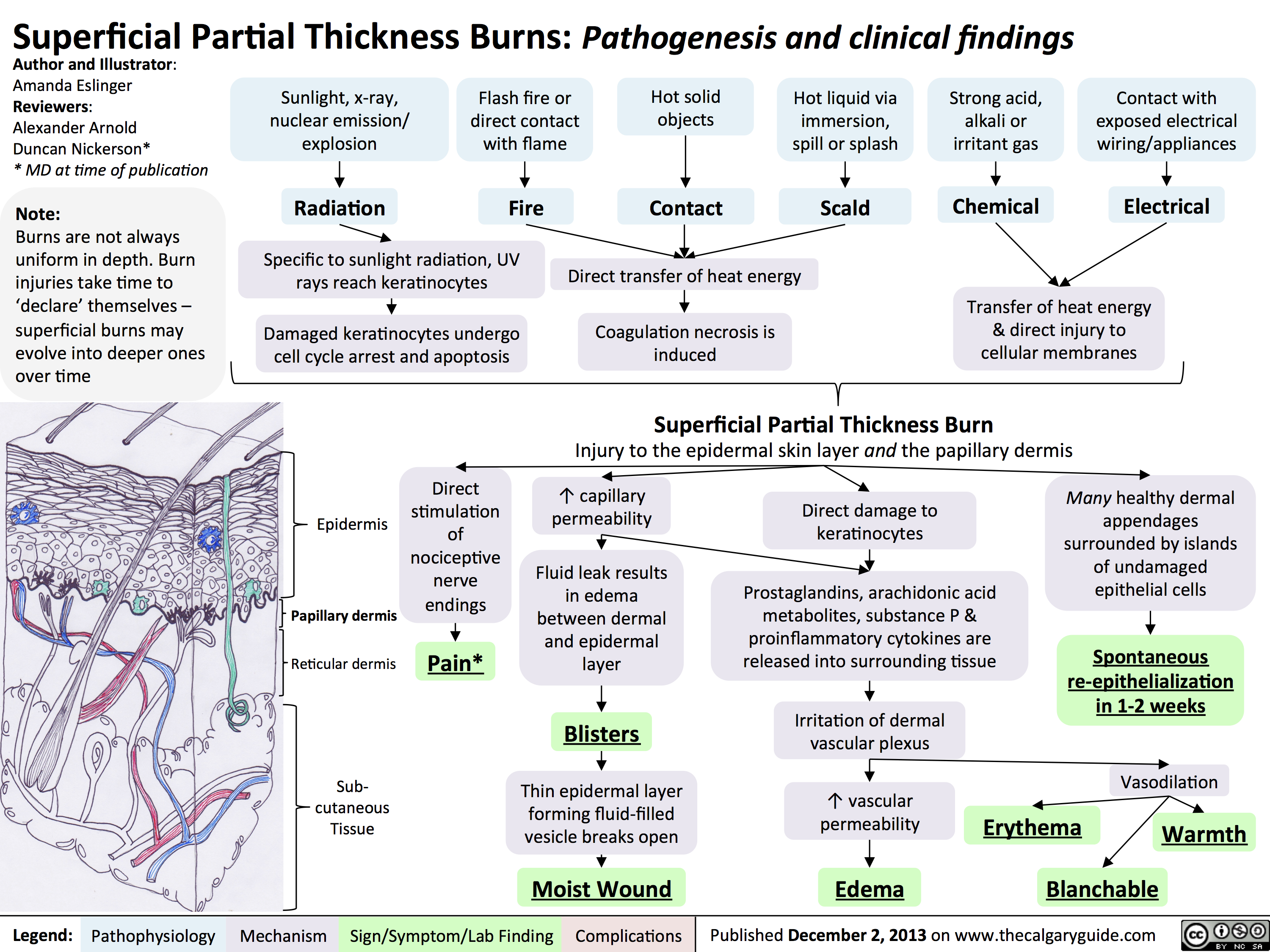
- First Degree Burn: superficial to partial thickness burns that burn the epidermis, resulting in erythema (pink to red) and mild to moderate pain. The most common type of first degree burn is a sunburn.
- If rubbed, the skin does not separate from the underlying dermis. This is known as a negative Nikolsky’s sign.
- Superficial: the blood supply to the dermis is still intact. (Saunders)
- Partial-thickness: Blood supply is reduced. The burn is painful and sensitive to cold air. (Saunders)
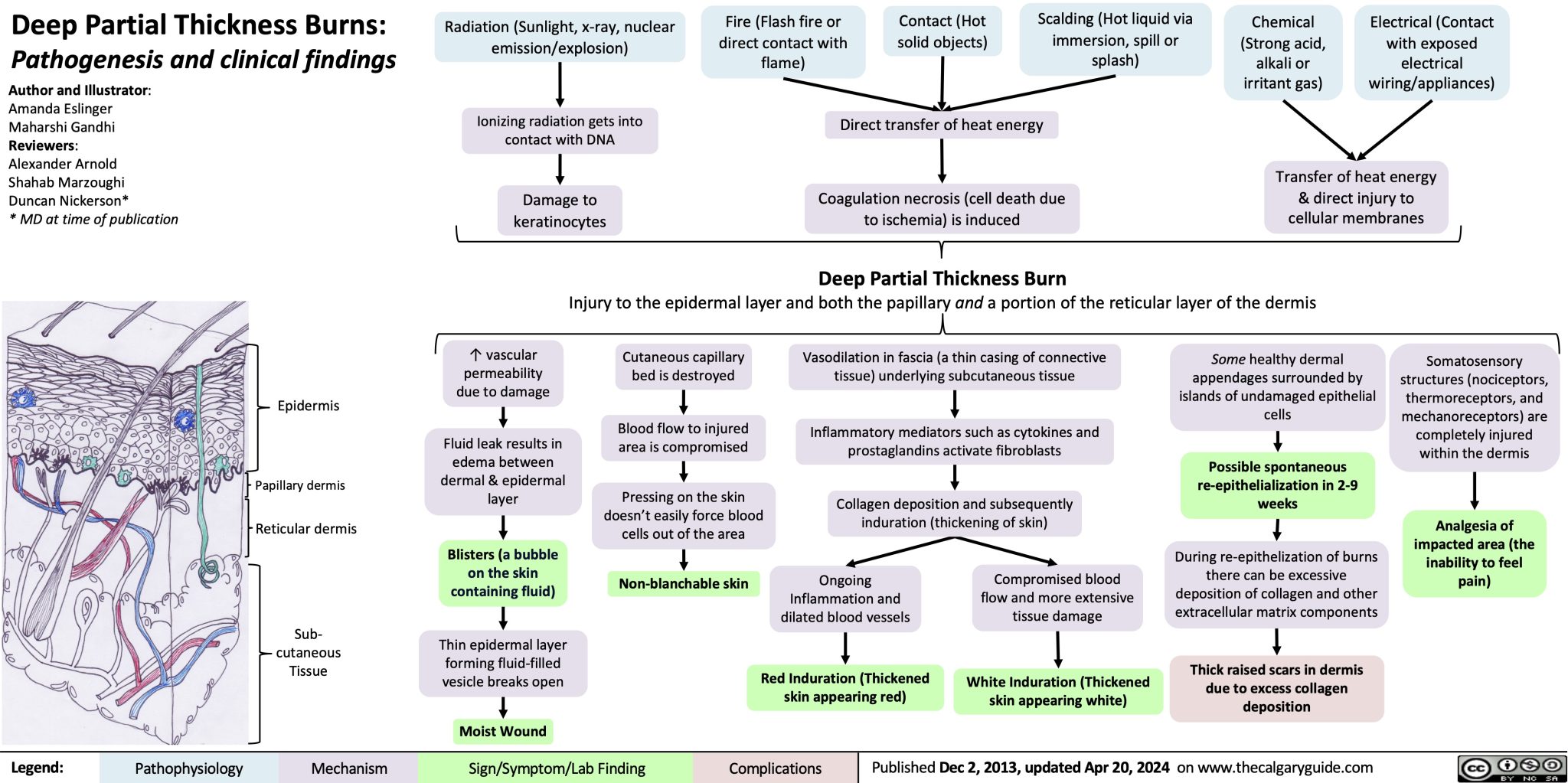
- Second Degree Burn: deep partial thickness burns that penetrate deep into the dermis. This results in blistering, a “weeping” appearance of the injury (due to serous leakage from peripheral microcirculation), edema, and severe pain. These are the types of burn to result from scalding and flash flames.
- Third Degree Burn: full thickness burns that reach the subcutaneous layer. The skin appearance varies from pale-white to red, brown, or charred. The patient experiences no pain (Insensate) due to the destruction of nerve fibers. These may be caused by extreme exposure to thermal burns or due to an electrical or chemical burn. Destruction of peripheral microcirculation results in a dry, leathery wound.
- Blisters no longer form because of the thick dead tissue layer that sticks to underlying tissue.
- Fourth Degree Burn: burns that extend into deep tissue, muscle, or bone (deep burn necrosis). Sensation is completely absent; there is no pain from destruction of nerve endings. Eschar is hard and inelastic. Healing will take months and grafts are required. (Saunders)
| First Degree | Second Degree | Third Degree | Fourth Degree |
|---|---|---|---|
| Superficial | Partial Thickness | Full Thickness | Fat, Fascia, Muscle, and/or Bone |
| Sunburn, Low-intensity flash, Superficial scald | Scalds, Flash flame, Contact | Flame, Prolonged exposure to hot liquids, Electric current, Chemical, Contact | Prolonged exposure or high-voltage electrical injury |
| Epidermis | Epidermis, portion of dermis | Epidermis, dermis, and sometimes subcutaneous | Deep tissue, muscle and bone |
| Tingling Hyperesthesia Pain soothed by cooling Peeling Itching | Pain Hyperesthesia Sensitive to air currents | Insensate Shock Myoglobinuria and possible hemolysis Possible contact points | Shock Myoglobinuria and possible hemolysis |
| Reddened; blanches with pressure; dry Minimal or no edema Possible blisters | Blistered, mottled red base; disrupted epidermis; weeping surface Edema | Dry; pale white, red brown, leathery, or charred Coagulated vessels may be visible Edema | Charred |
| Complete recovery (no scarring) within a few (3 to 6) days: oral analgesia, cool compress, skin lubricants | Recovery in 2–3 weeks Some possible scarring and depigmentation; may require grafting if healing is prolonged | The wound will not heal by reepithelialization. Dry, hard, leathery eschar may slough off or be removed. Grafting is necessary. Scarring and loss of contour and function. | Healing may take months or may no longer occur—amputations are likely. Grafting with no benefit given depth and severity of wound(s). |
Body Surface Area Formulas
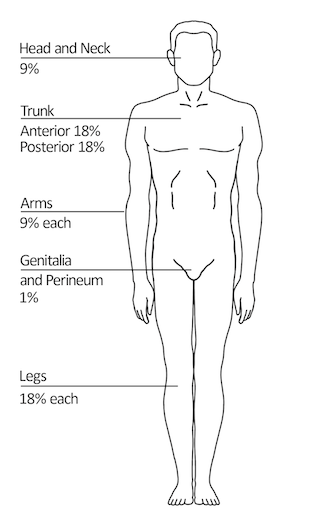
Various methods are utilized to estimate the total body burn surface area (TBSA) affected by burns; among them are the rule of nines, the Lund and Browder method, and the palmer method.
- Rule of Nines: the most common method of estimating the extent of burns in adults is the rule of nines. Be critical in determining percentages: presentations may involve only the anterior portion of a body part—this would halve the body part’s respective percentage. For example, the “anterior chest” would be ~9% as the anterior trunk is divided between the chest and the abdomen; “a circumferential burn of the left upper arm” would be approximately 4.5%, as it involves both the front and back of the upper arm.
- Alterations are required for pediatric clients due to differing proportions—the head is larger and carries more surface area, making it count for 18% of TBSA. The genitals are at 0%, and the lower extremities are brought down to 14%. The trunk and arms remain the same.
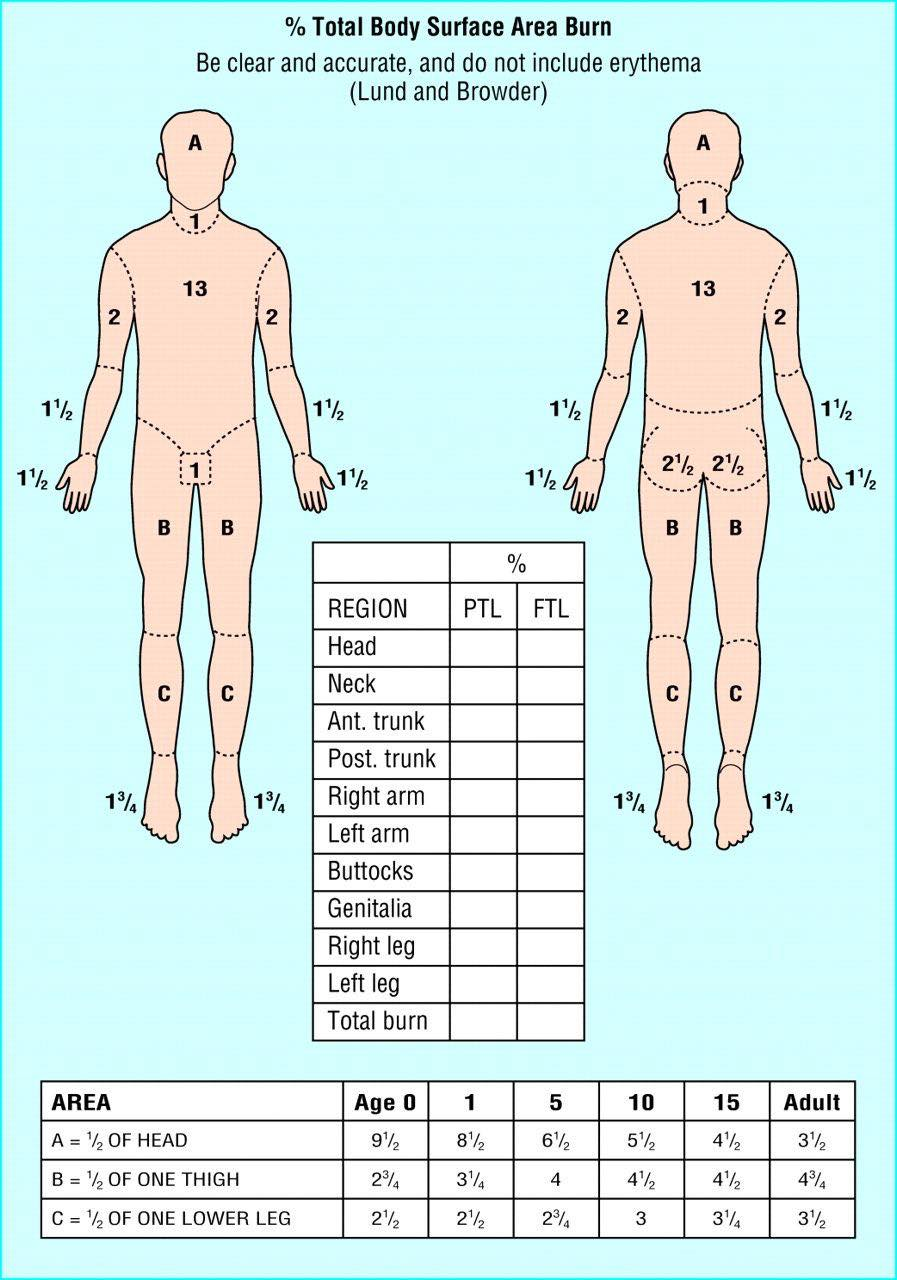
- Lund and Browder’s Method is a more precise method of estimating the extent of a burn. It recognizes the percentage of surface area of various anatomic parts, especially the head and legs, as it relates to the age of the patient. This small segmentation allows for a reliable estimate of TBSA burned. This utilizes a chart, as requires a more skilled assessment.
- Palmer Method is used for scattered burns, or very large burns with minimal sparing (by subtracting from 100%). It allows for an expeditious method to determine the extent of injury. The size of the patient’s hand, including the fingers, is approximately 1% of that patient’s TBSA.
Severe Injury
Any injuries that affect more than approximately 20% TBSA should be considered severe, as they produce both local and systemic effects.
Pathophysiology
| System | Physiologic Changes |
|---|---|
| Cardiovascular | Cardiac depression, edema, hypovolemia |
| Pulmonary | Vasoconstriction, edema |
| Gastrointestinal | Impaired motility and absorption, vasoconstriction, loss of mucosal barrier function with bacterial translocation, increased pH |
| Kidney | Vasoconstriction |
| Other | Altered thermoregulation, immunodepression, hypermetabolism |
Burn injury is the result of a chemical exposure or heat transfer from one site to another, causing tissue destruction through coagulation, protein denaturation, or ionization of cellular contents. The burn wound is not homogeneous; rather, tissue necrosis generally occurs at the center of the injury with regions of tissue viability toward the periphery:
- Zone of Coagulation: the central area of the wound where cells coagulate and become necrotic.
- Zone of Stasis: the area surrounding the zone of coagulation where injured cells remain viable but will undergo necrosis within 24 to 48 hours with persistent ischemia due to compromised blood supply and inflammation.
- Zone of Hyperemia: the outermost zone of the burn injury, sustaining minimal injury, able to recover spontaneously over time.
Burn Variants
- Burns affecting deep tissues involve the release of local mediators, changes in blood flow, tissue edema, and infection, causing progression in severity of the initial burn injury.
- Radiation exposure resulting in burns causes damage by two means: thermal exposure and damage to the cellular deoxyribonucleic acid (DNA), which may be localized or affect the whole body. Depending on the dose received, this may result in further morbidity or mortality.
The following slides are all content of The Calgary Guide to Understanding Disease, a free resource.

Cardiovascular Alterations
- Immediate decrease in cardiac output that precedes the loss of plasma volume.
- Systemic inflammation causes the release of free oxygen radicals that increase capillary permeability, causing increased plasma loss and subsequent peripheral edema as water migrates to the interstitium.
- As a compensatory response to intravascular fluid loss, the sympathetic nervous system releases catecholamines, resulting in an increase in peripheral resistance (vasoconstriction) and an increase in pulse rate that further decreases tissue perfusion.
- Due to vasoconstrictive compensatory responses secondary to plasma volume loss through capillary leak, the workload of the heart and oxygen demand increase.
- Hypovolemia is the immediate consequence of ensuing plasma volume loss and results in decreased perfusion and oxygen delivery to organs and tissues.
- As capillary leakage continues, vascular volume, cardiac output, and blood pressure decrease. This is the onset of early burn shock. Burn shock is initially a type of hypovolemic shock secondary to intravascular volume loss.
- If unmanaged with fluid resuscitation, distributive shock occurs.
Period of Maximal Leakage
Generally, the greatest volume of intravascular fluid leak occurs in the first 24 to 36 hours after the burn injury, peaking at approximately 6 to 8 hours after the initial burn injury. As the capillaries begin to regain their integrity, burn shock resolves and fluid shifts back into the vascular compartment. Intrinsic diuresis will begin and continue for several days to 2 weeks in the previously healthy adult.
Urinary output is the most reliable and most semsitive noninvasive assessment parameter for cardiac output and tissue perfusion. (Saunders)
Fluid and Electrolyte Alterations
In burns greater than 20% TBSA, inflammatory mediators stimulate local and systemic reactions resulting in extensive shift of intravascular fluid, electrolytes, and proteins into the surrounding interstitium. Edema forms rapidly after a burn injury.
- A superficial burn will cause localized edema to form within 4 hours, whereas a deeper burn will continue to form edema up to 18 hours post injury.
- Reabsorption of edema begins about 4 hours post injury and is complete approximately 4 days postburn injury.
- Hyperkalemia may occur immediately after a burn injury from massive cell destruction. Hypokalemia may occur later with fluid shifts and inadequate potassium replacement.
- Serum sodium levels vary in response to fluid resuscitation. Hyponatremia may be present from plasma loss or may occur during the first week of the acute phase, as water shifts from the interstitial space and returns to the vascular space (hemodilution).
Acute Compartment Syndrome
As the taut, burned tissue becomes unyielding to the edema beneath its surface, it begins to act like a tourniquet, especially if the burn is circumferential. As edema increases, pressure on small blood vessels in the distal extremities obstructs blood flow resulting in consequent tissue ischemia and potentially acute compartment syndrome. In mild cases, a simple elevation of the extremity may help. In severe cases, an escharotomy or fasciotomy may be required to relieve constricted muscle and restore tissue perfusion.
Pulmonary Alterations
Inhalation injuries, caused by inhalation of thermal and/or chemical irritants, are categorized as upper airway injury (above the glottis) or lower airway injury (below the glottis). Often, lower airway injuries are those produced by chemical inhalation. This is one of the highest determinants of mortality, along with the age of the patient and burn size.
- Upper Airway Injury is obstructive. Direct thermal injury produces erythema, edema, blistering, and ulcerations to the upper airway mucosa. Edema that can lead to upper airway obstruction can also be caused by burns to the face or neck. Upper airway obstruction is common in the first 24 to 48 hours. Protective intubation is often warranted to maintain patency of the airway.
- Lower Airway Injury often results from the inhalation of incomplete combustion or noxious gases, and is a common source of death at the scene of a fire. Smoke inhalation causes a loss of ciliary action, triggers an inflammatory response causing hypersecretion, producing severe mucosal edema and potential bronchospasm. A reduction in alveolar surfactant production produces atelectasis in the parenchyma. Expectoration of carbon particles in the sputum is a cardinal sign of lower airway inhalation injury. Aggressive pulmonary toileting (huff coughing, chest physiotherapy, suctioning, expectorants, etc.) is critical to maintain airway patency and clear resulting viscous sputum.
Noxious Gases
Noxious gases, such as carbon monoxide (CO) and hydrogen cyanide, contribute to lower airway injuries.
CO poisoning is a factor in most fatalities at the scene of a fire as it combines with hemoglobin 200 times more readily than oxygen does, forming carboxyhemoglobin. Treatment is administration of 100% oxygen to displace the CO molecules bound to hemoglobin, bringing the half-life of CO down to 45 minutes. (Brunner & Suddarth) Clinical manifestations of CO poisoning depends on the blood level of carboxyhemoglobin. A normal level can range from 1 to 10%. 11 to 20% results in a headache, flushing, decreased visual acuity, decreased cerebral functioning, and slight breathlessness. 21 to 20% produces nausea and vomiting, tinnitus and vertigo, decreased level of consciousness, pallor or slight cyanosis, hypotension, and tachycardia and arrythmias. 41 to 60% results in a coma, seizures, and cardiopulmonary instability. Any higher results is most likely fatal. (Saunders)
Hydrogen cyanide (produced from incomplete combustion of many household items) is a rapid systemic toxin, producing similar symptoms to CO poisoning and can include shortness of breath, headache, vertigo, confusion, and mucous membrane irritation. Cardiopulmonary effects initially cause a hyperdynamic response followed by bradycardia and hypotension leading to death. Persistent lactic acidosis after resuscitation is a sign of hydrogen cyanide poisoning.
The determination of inhalation injury may be made from a history of the injury—if a flame injury occurred in an enclosed space, if the patient’s facial hair is singed, or if expressed sputum is carbonaceous (appears black due to the presence of soot). Bronchoscopy is considered the standard test for definitive diagnosis as initial chest x-rays appear normal.
Assessment Findings in a Smoke Inhalation Injury
- Facial burns
- Erythema
- Swelling of the oropharynx and nasopharynx
- Singed nasal hairs
- Flaring nostrils
- Stridor, wheezing, and dyspnea
- Hoarse voice
- Sooty (carbonaceous) sputum and cough
- Tachycardia
- Agitation and anxiety
Bronchoconstriction (caused by a release of histamine, serotonin, and thromboxane) and chest constriction secondary to circumferential torso burns can contribute to deterioration. Even without pulmonary injury, hypoxia may be present from catecholamines and hypermetabolism. Administration of supplemental oxygen will ensure that adequate oxygen is available for body tissues. For full-thickness burns encircling the thorax, an escharotomy may be indicated.
Kidney Alterations
Kidney function may be altered as a result of decreased blood volume postburn injury due to the compensatory response to intravascular volume loss. Adequate fluid volume replacement can restore renal blood flow, increasing the glomerular filtration rate and urine volume.
Hemolysis may result in free hemoglobin in the urine. Muscle damage may result in myoglobinuria, turning urine red. Both of these can result in occlusion of the renal tubules, which can cause acute tubular necrosis and acute kidney injury. Fluid resuscitation helps by ensuring adequate blood flow will reach the kidneys. Kidney injury may also result from increased abdominal pressure.
Immunologic Alterations
The skin is the largest barrier to infection. A burn injury continually exposes the patient to the environment, and itself produces a systemic release of cytokines and other substances that cause leukocyte and endothelial cell dysfunction. This necessitates an infection-controlled environment to protect the patient and minimize exposure to potentially harmful organisms.
Thermoregulatory Alterations
Integumentary loss also causes an inability to regulate body temperature resulting in various complications. Patients with burn injuries often exhibit low body temperatures in the early hours after injury not necessarily due to initial first aid, which may include cooling of the wounds, but more likely from the amount of TBSA involved, the IV resuscitation fluids administered, and exposure resulting in increased evaporative heat loss. Burn centers often have additional heating sources to help maintain the patient’s body temperature through environmental warming.
Gastrointestinal Alterations
The most common gastrointestinal alterations in patients with burns are paralytic ileus (absence of intestinal peristalsis), Curling’s ulcer, and translocation of bacteria. Liver and pancreatic alterations may also occur.
- Paralytic ileus manifests as decreased peristalsis and bowel sounds. Gastric distention and nausea may lead to vomiting; therefore, gastric decompression is advised.
- Curling’s ulcer is gastric or duodenal erosion caused by ischemia of the stomach lining. Gastric bleeding secondary to massive physiologic stress may be signaled by occult blood in the stool, regurgitation of “coffee-ground” material from the stomach, or bloody vomitus.
- Colonization of pathogenic microorganisms can be avoided by maintaining intestinal barrier function with probiotics.
- Liver damage results from hepatic edema, apoptosis, insulin resistance associated with metabolic derangements, and development of a fatty liver.
- Acute pancreatitis is common in severe burn injuries, resulting in a threefold increase in amylase or lipase, feeding intolerance, or abdominal pain.
- Abdominal Compartment Syndrome (ACS) can occur due to the large volumes of fluid required for resuscitation and eschar formation on the abdominal walls, decreasing abdominal wall compliance. Increased pressure in the abdominal cavity contributes to GI tract and abdominal organ ischemia. Early laparotomy has been studied as a definitive treatment for ACS.
Electrical Burns
Electrical Injuries produce devastating and complex burns. Because of conduction into the body, visual inspection is not predictive of burn size and severity. Fluid resuscitation based on TBSA is inaccurate for this type of injury. This includes injuries such as flash injury, conductive injury, and lightning injury.
- Flash injuries is due to an electrical flash that generates light and heat. Clothing may ignite and damage is primarily due to heat. Patients with flash injuries have shorter lengths of stay than those with conductive injuries.
- Conductive injuries occur when electricity travels through the body. Conduction itself generates heat, causing damage to tissues adjacent to the path of the current. Entrance and exit wounds or contact points can help identify the probably current path and therefore anticipated tissue and organ involvement. Visual inspection is inadequate. Compartment syndrome may also occur due to edema and attempts at fluid resuscitation. This may require decompressive therapies such as fasciotomies, nerve releases, ocular releases, and laparotomies.
- Lightning injuries carry approximately 10% mortality rate, with many survivors reporting permanent morbidity. Deep polarization of the entire myocardium poses the risk of possible cardiac arrest. Respiratory arrest may also occur as the electric current can temporarily inactivate the brain’s respiratory center.
Due to the inadequacy of TBSA as a metric for required fluid resuscitation, intravenous fluid administration is titrated to a target urine output per hour. Serum creatinine kinase levels may be used to determine the degree of muscle injury in the early phases of care. Serum myoglobin and urine myoglobin levels may be monitored as indicators of the need for continued resuscitation.
In patients with myoglobinuria, common with muscle damage, kidney failure is a potential risk and warrants a higher target urine output per hour until the urine is no longer red. It is also common practice to add 50 mEq of sodium bicarbonate per liter of IV fluid in an effort to assist in alkalinizing the urine.
Surgical treatment is as complex as the injury itself. Vasculature is commonly affected, resulting in progressive necrosis over time from vascular insufficiency. Sequential surgical débridement may be necessary, using caution to preserve viable tissue.
Management of Burn Injury
Burn recovery generally occurs in three phases: emergent/resuscitative, acute/intermediate, and rehabilitation. Although priorities exist for each of the phases, assessment and management of problems and complications will overlap. The following is a summary:
| Phase | Duration | Priorities |
|---|---|---|
| Emergent, Resuscitative | From onset of injury to completion of fluid resuscitation. | - Primary survey: ABCDE - Prevention of shock - Prevention of respiratory distress - Detection and treatment of concomitant injuries - Wound assessment and initial care |
| Acute, Intermediate | From beginning of diuresis to near completion of wound closure. | - Wound care and closure - Prevention or treatment of complications, including infection - Nutritional support |
| Rehabilitation | From major wound closure to return to individual’s optimal level of physical and psychosocial adjustment. | - Prevention and treatment of scars and contractures - Physical, occupational, and vocational rehabilitation - Functional and cosmetic reconstruction - Psychosocial counseling |
Emergent/Resuscitative Phase
- The first step in management is to remove the patient from the source of injury and to stop the burning process while preventing injury to the rescuer.
- Priorities include establishing an airway, supplying oxygen (100% if CO poisoning is suspected), inserting at least one large-bore IV catheter for fluid administration, and covering the wound with a clean, dry cloth or gauze.
- Continuous irrigation of chemical injury must begin immediately.
- An immediate primary survey is performed assessing the ABCDEs: airway, breathing, circulatory and cardiac status, disability (including neurologic deficit), and expose and examine (while maintaining a warm environment).
- Airway patency and breathing must be assessed during the initial minutes of emergency care. If qualified personnel and equipment are available and the patient with burns has severe respiratory distress and/or airway edema, the rescuers must insert an endotracheal tube and initiate mechanical ventilation.
- The secondary survey focuses on obtaining a history, the completion of the total body systems assessment, initial fluid resuscitation, and provision of psychosocial support of the conscious patient.
Emergency Procedures at the Burn Scene
- Extinguish the flames or remove the source. “Stop, drop, and roll”, or if nonmobile, “Stop, sit, and pat”.
- If the burn source is electrical, the disconnect it safely first before approaching the patient.
- Cool the burn. The burned area and adherent clothing are soaked with cool water.
- Never apply ice.
- The use of cool soaks should not last for more than 20 minutes as this may worsen tissue damage and lead to hypothermia especially in large burns.
- Remove restrictive objects. Nonadherent clothing should be removed immediately. Adherent clothing is left in place once cooled. Other clothing and all jewelry (including piercings) are removed to allow for assessment and prevent constriction secondary to rapidly developing edema.
- Cover the wound. This should be done as quickly as possible to minimize bacterial contamination, maintain body temperature (↓ evaporative heat loss), and decrease pain caused by air currents.
- Any clean, dry cloth can be used as an emergency dressing.
- Ointments and salves should not be used.
- Other than the dressing, no medication or material should be applied to the burn wound at the scene.
- Irrigate chemical burns. Chemical burns will continue to cause damage as long as the chemical remains on the patient’s skin. Copious amounts of continuous running water is used to irrigate the burn.
- If the chemical agent is dry, it may be brushed off. All potentially contaminated clothing are removed and body parts that have come in contact with the chemical are immediately rinsed.
- If the chemical agent is in or near the eyes, the eyes should be flushed with cool, clean water immediately and copiously. Contact lenses, if present, should be removed.
Medical Management
Initially, the patient is transported to the nearest emergency department so that lifesaving measures can be initiated. Early referral to a burn center is then made if indicated.
- Initial priorities remain airway, breathing, and circulation. For mild pulmonary injury, 100% humidified oxygen is given, and the patient is encouraged to cough (pulmonary toileting) so that secretions can be expectorated or removed by suctioning. For more severe situations, it may be necessary to remove secretions by bronchial suctioning and administer bronchodilators and mucolytic agents. Continuous monitoring of airway patency is critical; edema formation and toxic effects of smoke inhalation can cause rapid deterioration of a previously stable airway.
- Once urgent respiratory needs are appropriately addressed, fluid resuscitation is initiated. In patients with burns greater than 20% TBSA, fluid resuscitation addresses the intravascular volume deficit to improve tissue and organ perfusion caused by plasma loss, with the least amount of fluid possible. Daily weights and trends in laboratory test results require close monitoring in the immediate postburn (resuscitation) period to monitor fluid status. Shock, ischemic complications, and multiple organ dysfunction syndrome (MODS) occur with underresuscitation. Overresuscitation results in heart failure and pulmonary edema.
- Peripheral IV access may be adequate for initial fluid administration, but central venous access is recommended to large volumes to be administered. Once the TBSA is calculated, fluid resuscitation with lactated Ringer (LR) should be initiated using America Burn Association (ABA) resuscitation formulas. LR is the crystalloid of choice because its pH and osmolality most closely resemble human plasma.
- The ABA (2018) fluid resuscitation formula for adults within 24 hours post thermal or chemical burn is as follows for second, third, and fourth degree burns: 2 mL LR/kg/%TBSA (kg referring to patient body weight).
- For adults with electrical burns of second, third, and fourth degree, 4 mL LR/kg/%TBSA is used instead. This is known as the Parkland (Baxter) Formula. The Modified Parkland Formula adds on 15 mL/m² of TBSA.
- Alternatively, the Modified Brooke formula infuses 5% albumin in isotonic saline and Lactated Ringer’s without dextrose at 0.5 mL to 15 mL/kg/%TBSA.
- Timing is one of the most important considerations in calculating fluid needs in the first 24 hours post burn. The starting point is the time of injury—not the time of arrival to the treating facility (ABA, 2018). The infusion is regulated so that half of the total calculated volume is given in the first 8 hours postburn injury. The second half of the calculated volume is infused over the next 16 hours.
- While these formulas provide a general guideline, infusion should still be titrated hourly as indicated by physiologic monitoring the patient’s response. Urinary output continues to be the standard for assessing patient response to fluid resuscitation. An appropriate urine output in adults is 0.5 to 1 mL/kg/hr, indicating resuscitation in thermal and chemical injuries. In electrical injuries, a urine output of 75 to 100 mL/hr is desired.
- After circulatory status has been established, the patient is assessed for cervical spine and/or head injuries, if suspected. All clothing and jewelry are removed because they may retain chemicals, heat, or become constrictive as edema develops. If the eyes may have been damaged, consultation with an ophthalmologist may be beneficial.
- The patient’s temperature must be monitored because hypothermia may develop rapidly, and manipulation of the environment may be necessary. A temperature less than 35°C (95°F) causes vasoconstriction, which may increase tissue ischemia and necrosis.
- An indwelling urinary catheter is inserted to permit accurate monitoring of urine output and fluid needs and as a measure of kidney function for patients with moderate to severe burns.
- If the burn exceeds 20% to 25% TBSA, a nasogastric tube is inserted and connected to low intermittent suction. All patients who are intubated should have a nasogastric tube inserted to decompress the stomach, and to prevent vomiting and aspiration. Often, patients with large burns become nauseated as a result of the GI effects of the burn injury, such as paralytic ileus, and the effects of medications such as opioids.
- Clean sheets are placed under and over the patient to protect the burn wound from contamination, maintain body temperature, and reduce pain caused by air currents passing over exposed nerve endings.
- Analgesia is given in small repeated doses, which is crucial for pain reduction in the emergent phase.
- A baseline electrocardiogram and continuous cardiac monitoring is indicated for patients with electrical burns.
- Tetanus prophylaxis is given if the patient’s immunization status is not current or unknown because burns are considered contaminated wounds.
Nursing Management
The burn wound is a secondary consideration to stabilization of airway, breathing, and circulation. The nurse monitors respiratory status closely, and pulses are evaluated, particularly in areas of circumferential burn injury to an extremity. Initially, cardiac monitoring is indicated if the patient has a history of heart cardiac disease, electrical injury, or altered respiratory conditions. The nurse should monitor vital signs with knowledge of expected abnormalities consistent with burn injury such as tachycardia, and tachypnea.
- Blood Pressure: If all extremities are burned, determining blood pressure may be difficult. If necessary, a blood pressure cuff may be placed around a patient’s burned extremity. Clean dressing applied under the blood pressure cuff protects the wound from contamination. Increasing edema makes blood pressure difficult to auscultate. Doppler (ultrasound) assistance or a noninvasive electronic blood pressure device may be helpful. In severe burns, an arterial catheter is preferred for blood pressure measurement and is simultaneously helpful for collecting blood specimens.
- Peripheral Pulses are checked frequently either by palpation or the use of a Doppler. Elevation of burned extremities above the level of the heart is indicated for edema reduction.
- Large-bore IV catheters (e.g., 16 to 18 gauge) and an indwelling urinary catheter are inserted, if not already in situ, and the nurse’s documentation must include hourly assessment of fluid intake and urine output.
Urine Characteristics
Red-colored urine suggests the presence of hemochromogens from damage to red blood cells and myoglobin, the by-product of muscle damage. This anomaly is associated with deep burns caused by electrical injury or prolonged contact with heat or flame.
Glycosuria is a common finding in the early postburn hours due to the release of liver glycogen stores in response to stress.
The nurse assists with calculating the patient’s expected fluid requirements and monitoring the patient’s response to fluid resuscitation. Nursing responsibilities consists of appropriate fluid administration, strict monitoring of intake and output, monitoring the patient’s response, and notifying the treatment team of significant assessment findings and any abnormal laboratory values.
- To help guide treatment, the following are essential: documentation of body temperature, body weight, and pre-burn weight; history of allergies, tetanus immunization, past medical and surgical history, and current illnesses; and a list of current medications.
- The nurse performs a head-to-toe assessment, focusing on signs and symptoms of concomitant illness, associated trauma, or developing complications.
- Assessing the extent of the burn wound using the rule of nines or facilitated with anatomic diagrams (described previously) is performed. Additionally, the nurse works with the primary provider to clinically assess and document the initial areas of full- and partial-thickness injury.
Nursing Diagnoses, Goals, and Interventions
- Impaired gas exchange associated with carbon monoxide (CO) poisoning, smoke inhalation, and upper airway obstruction. Goal: Maintenance of adequate tissue oxygenation.
- Provide 100% humidified oxygen
- Assess breath sounds, and respiratory rate, rhythm, depth, and symmetry of chest excursion. Monitor for hypoxia.
- Observe for erythema or blistering of the lips or buccal mucosa; singed nasal hairs; burns of the face, neck, or chest; increasing hoarseness; or soot in sputum or tracheal tissue in respiratory secretions.
- Monitor arterial blood gas values, pulse oximetry readings, and carboxyhemoglobin levels.
- Prepare to assist with intubation and escharotomies of chest.
- Impaired airway clearance associated with exposure to smoke. Goal: Maintain patent airway and adequate airway clearance.
- Maintain patent airway through proper patient positioning, removal of secretions, and artificial airway if needed.
- Provide humidified oxygen as prescribed.
- Encourage the patient to turn, cough, and deep breathe. Encourage patient to use incentive spirometry. Perform endotracheal suction as needed.
- Hypovolemia associated with increased capillary permeability and evaporative losses from the burn wound. Goal: Restoration of optimal fluid and electrolyte balance and perfusion of vital organs.
- Monitor vital signs, hemodynamics, and urine output, as well as record strict intake and output and daily weights.
- Maintain IV lines and regulate fluids at prescribed and appropriate rates following urine output.
- Observe for symptoms of deficiency or excess of serum sodium, potassium, calcium, phosphorus, and bicarbonate.
- Elevate head of patient’s bed and burned extremities, if not contraindicated. This promotes venous return.
- Notify primary provider immediately of decreased urine output and hemodynamic changes.
- Hypothermia associated with loss of skin microcirculation and open wounds. Goal: Maintenance of adequate body temperature.
- Assess core body temperature frequently.
- Provide a warm environment by increasing room temperature or adjust therapies as needed (overbed warmers, heat lamps, etc.)
- Work quickly when wounds must be exposed.
- Acute pain associated with chemical or physical injury. Goal: Control of pain.
- Assess pain level with a pain intensity scale. Differentiate restlessness due to pain from restlessness due to hypoxia.
- Administer IV antispasmodic agents as prescribed and assess for effectiveness.
- Provide emotional support and reassurance. Fear and anxiety increase the perception of pain.
- Anxiety associated with fear and the emotional impact of burn injury. Goal: Minimization of patient’s and family’s anxiety.
- Assess patient’s a family’s understanding of burn injury, coping skills, and family dynamics.
- Explain all procedures to the patient and the family in clear, simple terms.
- Administer prescribed antianxiety medications if the patient remains extremely anxious despite nonpharmacologic interventions.
| Complication | Nursing Interventions |
|---|---|
| Acute Respiratory Failure | Assess for increasing dyspnea, stridor, changes in respiratory patterns. Monitor pulse oximetry, arterial blood gas values, and chest x-ray results. Signs of cerebral hypoxia are early manifestations of failing oxygenation: restlessness, confusion, difficulty attending to questions, or decreasing level of consciousness. Report deteriorating respiratory status immediately to primary provider. Prepare to assist with intubation or escharotomies as indicated. |
| Distributive Shock | Assess for decreasing urine output and alterations in vital signs and hemodynamics. Assess for progressive edema that appears as fluid shifts occur. Adjust fluid resuscitation in collaboration with the primary provider in response to physiologic findings. |
| Acute Kidney Injury | Monitor urine output, blood urea nitrogen, and serum creatinine levels. Assess the urine for hemoglobin or myoglobin. Administer increased fluids as prescribed. |
| Compartment Syndrome | Assess peripheral pulses frequently. Assess for warmth, capillary refill, sensation, and movement of extremity frequently. Remove blood pressure cuff after each reading. Elevate burned extremities if not contraindicated. Prepare to assist with escharotomies. |
| Paralytic Ileus | Auscultate for bowel sounds and check for abdominal distention. Maintain nasogastric tube on low intermittent suction until bowel sounds resume. |
| Curling’s Ulcer | Assess gastric aspirate and stools for blood. Administer histamine-2 blockers and/or antacids as prescribed. |
Acute/Intermediate Phase
The acute/intermediate phase of burn care follows the emergent/resuscitative phase and begins 48 to 72 hours after the burn injury. During this phase, attention is directed toward continued assessment and maintenance of respiratory and circulatory status, fluid and electrolyte balance, and GI and kidney function.
Infection prevention and control, burn wound care (e.g., wound cleaning and débridement, topical antibacterial/antimicrobial therapy, application of dressings, wound grafting), pain management, modulation of the hypermetabolic response, and early positioning/mobility are priorities in the acute/intermediate stage of recovery.
Medical Management
- Pulmonary complications are common in burn injury. Airway obstruction caused by upper airway edema can take as long as 48 hours to develop. Changes detected by x-ray and arterial blood gas analysis may occur as the effects of resuscitative fluid and the chemical reactions of smoke ingredients with lung tissues become evident.
- Diagnosis is largely based on history and clinical presentation, monitoring of arterial blood gases with carboxyhemoglobin levels, and direct observation of the airway by fiberoptic bronchoscopy (ABA, 2018).
- Stridor and dyspnea are ominous signs as they are late signs of impending airway obstruction.
- Elevation of the patient’s head may be helpful.
- Early protective intubation to maintain airway patency should be considered as obstruction can occur rapidly. However, intubation and mechanical ventilation are significant contributors to pulmonary infections. They are removed as soon as possible.
- Late pulmonary complications secondary to inhalation injuries include mucosal sloughing (peeling) of the airway and cast formation from cellular debris, which can lead to obstruction, increased secretions, inflammation, atelectasis, airway ulceration, pulmonary edema, and tissue hypoxia.
- Pneumonia, acute lung injury (ALI), and acute respiratory distress syndrome (ARDS) may also occur.
- Ventilator-associated pneumonia (VAP) is a common complication of any patient who is hospitalized and mechanically ventilated and is particularly exacerbated in the patient with an inhalation injury.
VAP Bundle
Current best practices can include the implementation of specific evidence-based bundle interventions that, when used together (i.e., as a “bundle”), improve patient outcomes. There are five key elements of the VAP bundle:
- Elevation of the head (30° to 45°)
- Daily “sedation vacations” and readiness to extubate. This involves decreasing sedative doses at a time of day when it is possible to assess the patient’s neurologic readiness for extubation. It is important to avoid the risk of self-extubation. This allows primary providers to determine whether extubation is possible.
- Peptic ulcer disease prophylaxis.
- Deep venous thrombosis (DVT) prophylaxis and its relationship to VAP is unclear. However, it is clear that evidence-based DVT prophylactic methods are shown to drop the rates of VAP.
- Daily oral care with chlorhexidine (0.12% oral rinses).
- Fluid shifting occurs as capillaries regain their integrity 48 or more hours after the burn. This shift is from the interstitial to the intravascular compartment, resulting in diuresis. With inadequate cardiac or kidney function, fluid overload may occur, and symptoms of heart failure may emerge.
- Administration of fluids and electrolytes continues cautiously during this phase of burn care due to fluid shifts, evaporative fluid loss from large burn wounds, and the patient’s physiologic responses to the burn injury. Blood components are given as needed to treat surgical blood loss and anemia.
- Hyperthermia is common in patients after burn shock resolves. A resetting of the core body temperature in patients who are severely burned results in a body temperature a few degrees higher than normal for several weeks after the burn. This can be compounded by body temperature increases from sepsis.
- Central venous, arterial, or specialty catheters (e.g., hemodialysis catheters, Zoll® catheters) may be required for monitoring hemodynamics.
- Early excision is one of the most important medical interventions. The presence of open wounds or invasive organisms trigger the response to a large burn injury, a systemic cascade of events. Excising the necrotic tissue can ameliorate this response and preserve viable underlying tissue.
Infection Prevention and Control
There are multifactorial reasons why patients with burns incur some of the highest risks of health care-associated infections (HAIs). The immune system becomes dysregulated, the wound provides a perfect medium for bacterial proliferation and conduit to the blood stream, the loss of the epidermal bladder, the presence of transmittable bacteria, and the ubiquity of mold species in the environment make it critical for the nurse to prioritize infection prevention in the plan of care. Required invasive procedures further undermine the body’s natural defenses.
Whether the burn wound is healing through spontaneous reepithelialization or is being prepared for skin grafting, protection from pathogens (bacteria, fungi, viruses from equipment, healthcare workers, environmental surfaces, or translocation) is crucial. Infection results in progressive erythema, warmth, tenderness, and malodorous exudates.
- Strict usage of barrier techniques
- Environmental cleaning with periodic cultures of patient care equipment (especially for hydrotherapy equipment)
- Application of appropriate topical antimicrobial agents and systemic antibiotic and antifungal agents (after careful use of culture sensitivities to battle antibiotic resistance). The use of broad prophylactic antibiotics is not supported by current research (2017).
- Early excision and closure of the burn wound.
- Control of hyperglycemia (insulin may be used even in patients without diabetes)
- Management of hypermetabolic response: collaboration with the dietitian or nutrition support team helps meet the needs of the patient, prescription of high-calorie nutritional supplements and vitamin and mineral supplements, accurate documentation of nutritional intake, insertion of feeding tube with continuous or bolus feedings of specific formulas if oral feedings are inadequate, daily weight is tracked to properly assess appropriate weight parameters and to attenuate catabolism of lean muscle mass.
Wound Cleaning
Proper management of burn wounds prevents wound deterioration. The goal is to remove nonviable tissue and wound exudate, and eliminate previously applied topical agents.
- Gentle cleaning with mild soap, water, and a washcloth can prevent infection by decreasing the bacteria and debris on the wound surface. Hair in and around the burn area, except the eyebrows, should be clipped short or shaved.
- Patients who are hemodynamically unstable are washed at bedside, while other can take showers. Whatever method employed, the goal is to protect the wound from acute proliferation of pathogenic organisms on the surface through mechanical washing to prevent invasion of deeper tissues until the wounds are closed through spontaneous healing or skin grafting.
- Patient comfort and ability to participate in the prescribed treatment are important considerations. During bathing, patient participation is encouraged to promote exercise and range of motion of the extremities.
- While cleaning, the nurse inspects for any signs of redness, breakdown, or local infection. This is also an opportunity for health education.
- Continuous assessment for hypothermia should be done. Water used for cleaning is maintained at 37.8°C (100°F) and the temperature of the room should be maintained between 26.6°C and 29.4°C (80°F and 85°F) to prevent hypothermia. Other assessment considerations include patient fatigue, changes in hemodynamic status, and pain unrelieved by analgesic medications or relaxation techniques.
Topical Antibacterial Therapy
Topical wound care is varied and individualized. The goal of topical therapy is to provide a dressing that is:
- Effective against gram-positive and gram-negative organisms and fungi.
- Penetrates the eschar but is not systemically toxic.
- Cost-effective, available, and acceptable to the patient.
- Easy to apply and remove, decreases the frequency of dressing changes, decreases pain, and minimizes nursing time.
No single topical medication is universally effective. Different agents at different times in the postburn period is best practice.
| Agent | Indication/Comment | Application | Nursing Implications |
|---|---|---|---|
| Antimicrobial ointment in general | Antibacterial coverage and promotion of a moist wound environment | Apply 1/16-inch layer of ointment with a clean glove daily. | Ensure removal of residual ointment at the time of wound cleaning prior to applying a new layer. Monitor closely for signs and symptoms of local infection. |
| Silver sulfadiazine 1% water-soluble cream | Bactericidal agent for many gram-positive and gram-negative organisms, as well as yeast and Candida albicans Minimal penetration of eschar | Apply 1/16-inch layer of cream with a clean glove 1–3 times daily. | Anticipate formation of pseudoeschar (proteinaceous gel), which can be removed. |
| Mafenide acetate 5% hydrophilic-based solution or cream | Antimicrobial agent for gram-positive and gram-negative organisms. Diffuses through eschar and avascular tissue (e.g., cartilage) | Apply twice a day with clean glove. | Is a strong carbonic anhydrase inhibitor and may cause metabolic acidosis. Application may cause considerable pain initially. |
| Silver nitrate 0.5% aqueous solution | Effective against most strains of Staphylococcus and Pseudomonas and many gram-negative organisms. Does not penetrate eschar. | Apply solution to gauze dressing and place over wound. Keep the dressing wet but covered with dry gauze and dry blankets to decrease vaporization. | Monitor serum sodium and potassium levels and replace as prescribed. Silver nitrate solution is hypotonic and acts as a wick for sodium and potassium. Protect bed linens and clothing from contact with silver nitrate, which stains everything it touches. |
| Silver-impregnated dressings (sheets or mesh) | Broad antimicrobial effects (depending on product) and delivers a uniform, antimicrobial concentration of silver ions to the burn wound. | Apply directly to wound. Cover with absorbent secondary dressing if needed. | May produce a pseudoeschar from silver after application. Can be left in place for several days (product specific). |
Wound Dressing
After topical agents are applied, the wound is covered with several layers of dry dressings with lighter dressing over joints to allow for mobility.
- Circumferential dressings should always be applied distally to proximally to promote return of excess fluid into the central circulation.
- In case of hand or foot burns, the fingers and toes should be wrapped individually to promote mobility and function while healing.
- Burns to the face may be left open to air once cleaned and the topical agent has been applied to maintain a moist environment. Careful attention ensures the topical agent does not come in contact with the eyes or mouth. A light, nonrestrictive dressing may be applied to the face to absorb excess exudate if needed.
- Occlusive dressings, bulky gauze, and a topical antimicrobial agent may be used over areas with new skin grafts to protect the new graft and promote an optimal condition for its adherence to the recipient site. These are ideally kept in place for 3 to 5 days to allow growth of the microcirculation into the new graft before removal for inspection of the graft. When occlusive dressings are applied, precautions are taken to prevent two body surfaces from touching to prevent skin maceration, pressure injury, and infection in moist, occluded areas.
- Dressings may also require modification to accommodate splints or other positioning devices. Functional body alignment positions are maintained by using splints or by regular repositioning of the patient.
Dressings can impede circulation if they are wrapped too tightly. Peripheral pulses must be checked frequently and burned extremities elevated. If the patient’s pulse is diminished, this is a critical situation and must be addressed immediately.
Dressings that adhere to the wound bed may be removed more comfortably and with less damage to healing tissue by moistening the dressing with water or saline during removal. The patient may participate in removing the dressings, providing some degree of control over the painful procedure. After removal, the wound is cleaned and débrided to remove any remaining topical agent, exudate, and nonviable tissue. Sterile scissors and forceps may be used to trim loose eschar and encourage separation of devitalized tissue.
During removal, the wound and surrounding skin are carefully inspected. Documentation should include color, odor, size, exudate, sign of reepithelialization, any changes from the previous dressing changes, and other key characteristics.
Wound Débridement
The goals of débridement is the removal of devitalized tissue or burn eschar in preparation for grafting and wound healing. It also removes any tissue contaminated by bacteria and foreign bodies, thereby protecting the patient from invasion of bacteria. There are four types of débridement:
- Natural Débridement: Devitalized tissue separates from the underlying viable tissue spontaneously. Bacteria present at the interface of the burned tissue and healthy viable tissue gradually liquefy the fibrils of collagen, a protein present in skin, tendon, bone, cartilage, and connective tissue, that hold the eschar in place. Proteolytic and other natural enzymes cause this phenomenon. The process may take weeks to months to occur.
- Mechanical Débridement: Surgical tools are used to separate and remove the eschar. This technique, performed by primary providers, specially trained nurses, or physical therapists, is usually performed with routine dressing changes. If bleeding occurs, hemostatic agents or pressure may be applied to achieve hemostasis.
- Dressing changes and wound cleaning aid the removal of wound debris. Wet-to-dry dressings (wet dressing applied to burn wound, then allowed to dry, then pulled off to remove tissue) are not advised for burn care because of the possibility of removing viable epithelial cells along with necrotic tissue. Wet-to-wet or wet-to-moist dressings may be used instead.
- Chemical Débridement: Topical enzymatic agents are available to promote débridement of burn wounds. These are often combined with topical antibacterial therapy as the topical enzymatic agents usually do not have antimicrobial properties. However, product instructions should be followed to ensure that each agent does not interfere with the other’s function.
- Surgical Débridement: Early surgical excision to remove devitalized tissue along with early burn wound closure has long been recognized as one of the most important factors contributing to survival in a patient with a major burn injury. This is done before the natural separation of eschar, as soon as possible after the burn once the patient is hemodynamically stable and edema has decreased. In ideal scenarios, the wound bed is immediately covered with a skin graft (if necessary) after excision. If it is not yet ready for a skin graft, a temporary biologic or synthetic dressing may be applied until an autograft can be successfully applied during a subsequent surgery.
Risks and Complications of Surgical Excision
The use of surgical excision carries with it risks and complications, especially with large burns. The procedure creates a high risk of extensive blood loss and lengthy operating and anesthesia times. Blood losses from the surgery, wound care, and ongoing hemolysis all exacerbate anemia. Blood transfusions may be required periodically to maintain adequate hemoglobin levels.
When conducted in a timely and efficient manner, surgical excision results in shorter lengths of stay and decreased risk of complications from invasive burn wound sepsis. Once débrided, granulation tissue fills the void created by the wound, creates a barrier to bacteria, and serves as a bed for epithelial cell growth. A wound covering is applied to keep the wound bed moist and promote the granulation process.
Wound Grafting
Patients with deep partial- or full-thickness burns (second, third degree) may be a candidate for skin grafting to decrease the risk of infection; prevent further loss of protein, fluid, and electrolytes through the wound; minimize evaporative heat loss; and reduce scarring.
- Special attention is warranted when grafting the face (for cosmetic, functional, and psychological reasons); functional areas, such as the hands and feet; and areas over joints. Grafting permits earlier function and reduces scar contractures (shrinkage of burn scar through collagen maturation).
- When burns are very extensive, the order in which areas are grafted is chosen based on the ability to achieve wound closure as soon as possible; therefore, the chest and abdomen or back may be grafted first to reduce the overall open wound size.
There are four types of grafts, based on the origin of the graft:
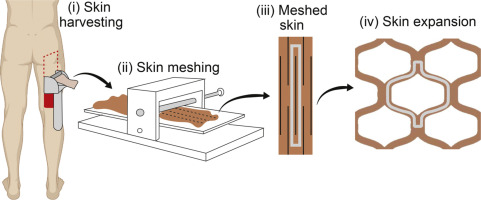
- Autografts are the preferred autologous method for definitive burn wound closure after excision. Autografts are the ideal means of covering burn wounds because the grafts are the patient’s own skin and therefore are not rejected by the patient’s immune system. They can be split-thickness, full-thickness, or epithelial grafts. Because the donor site (the area from which skin is taken) for a full-thickness graft includes both the epidermis and dermis, its use must be cautiously considered because the donor site will not be able to heal spontaneously.
- Split-thickness autografts are the most commonly used method and can be applied in sheets (layer of tissue), or applied as a mesh to cover a larger surface area. A mesh adheres more readily and prevents the accumulation of blood, serum, air, or purulent material under the graft that would prevent revascularization and adherence. The caveat is it contributes to scar formation as it heals. In large wounds, largely expanded grafts may be necessary with a compromise on cosmesis.
- The presence of blood, serum, air, fat, or necrotic tissue between the recipient site and the graft can result in a partial or total loss of the graft. Infection, mishandling, or sheer injury with mobilization or trauma during dressing changes accounts for most other instances of graft loss.
- Cultured epithelial autograft (CEA) has emerged as an important procedure in the management of massive burns (>90% TBSA) due to the insufficiency of donor sites . A full-thickness biopsy of the patient’s unburned skin is cultured to promote the growth of keratinocytes. In about three weeks, the final product is available for grafting. However, this tissue is extremely fragile and prone to graft loss. It also requires inordinately extended lengths of stay for the patient and is prohibitively expensive.


Care of the Graft and Donor Sites
- Graft Site: protection and immobility are key; occlusive dressings encased in bulky gauze wraps are commonly used for optimal healing. Splints may immobilize joints for newly grafted areas. Fragile grafts can be combined with homografts, xenografts, or synthetic dressings.
- The first dressing change is usually performed 3 to 5 days after surgery, or earlier if clinical signs of infection or bleeding are present.
- Position patients carefully to avoid disturbing the graft.
- Grafts on extremities should be elevated to reduce edema.
- The grafted area can be exercised 5 to 7 days after surgery. This may vary with individual protocols.
- Donor Site: the donor site is a clean, usually superficial wound in a surgical environment. A hemostatic agent is applied to promote hemostasis. Dressings are applied until the donor site heals spontaneously within 7 to 14 days in an adult who was previously healthy and nonsmoking. The site (usually a partial-thickness wound) is very painful, prone to infection, and very susceptible to pressure injury.
- Homografts (or allografts) and Xenografts are also referred to as biologic dressings and are intended as temporary wound coverage until autografting is possible. Homografts are obtained from recently decreased or living humans other than the patient. Xenografts consist of skin taken from animals (usually pigs). Because of this, the body’s immune response will eventually reject either of them as a foreign tissue.
- Biologic dressings can be left open to air or covered with a dressing. They provide many of the benefits of autografts (protection, decreased water and protein loss, barrier against bacteria, decrease pain) but only for some (varying) length of time.
- These may also be used as a test graft in preparation for autografting to determine if the wound bed will accept the graft—if the graft appears to be “taking”, the underlying tissue is likely ready for an autologous skin graft.
- Biosynthetic and Synthetic Dressings: biosynthetic drones may eventually replace temporary wound coverings. There are currently many products on the market, but they tend to be cost prohibitive for most patients and in most healthcare settings. Availability is also an issue.
Pain Management
A burn injury is considered one of the most painful types of trauma that a person can experience. The nature of the injury may expose nerve endings to the atmosphere; and the patient may require multiple procedures, débridements, surgeries, and treatments. Pharmacologic treatment for the management of burn pain includes the use of opioids, nonsteroidal anti-inflammatory drugs, anxiolytics (benzodiazepines), and anesthetic agents. Nonpharmacologic therapies used in conjunction with pharmacologic treatment is important for holistic care. These may include relaxation techniques, distraction, guided imagery, hypnosis, therapeutic touch, humor, music therapy, and virtual reality techniques.
Adequate pain management must address background, breakthrough, and procedural pain:
| Pain | Intervention |
|---|---|
| Background Pain: a continuous level of discomfort when the patient is inactive or not undergoing any procedures. | Long-acting analgesic agents provide uniform coverage for long-term discomfort. Small, escalating doses when initiating analgesia until the level of pain control is acceptable facilitates participation in recovery. |
| Breakthrough Pain: acute, intense, episodic pain that is generally related to an activity or movement of the affected area. | Short-acting analgesic agents are used to achieve pain control if needed. |
| Procedural Pain: discomfort that occurs with procedures such as daily wound treatments, invasive line insertions, and physical and occupational therapy. | Plan proper analgesia to facilitate comfort for the patient during the procedure. |
Modulation of Hypermetabolism
Burn injuries produce profound metabolic abnormalities fueled by the exaggerated stress response to the injury. The body’s response has been classified as hyperdynamic, hypermetabolic, and hypercatabolic. This increases the risk of infection and slows healing rate.
- Nutrition should be provided as soon as possible upon arrival to the burn center and may require placement of a nasogastric tube for adequate calorie delivery. The most important energy source is carbohydrates for patients with severe burns. Fat, although a required nutrient, should be provided in more limited quantities. When the oral route is used, high-protein, high-calorie meals and supplements are given. Consultation with a dietitian is useful to meeting nutritional needs. Daily calorie counts aid in assessing the adequacy of nutritional intake.
- Early excision and grafting ameliorates hypermetabolism by removing eschar, thereby lessening the effects of inflammatory mediators. This is one of the most important factors in modulating hypermetabolism.
- Appropriate manipulation of environmental temperatures decreases energy expenditure by the patient.
- Insulin therapy in patients with burns ins required to treat the hyperglycemia that occurs from accelerated gluconeogenesis and is beneficial in muscle protein synthesis.
- Oxandrolone, an anabolic steroid, is commonly given to patients with burns because it improves protein synthesis and metabolism.
- Propranolol decreases heart rate and blocks harmful catecholamine effects (e.g., vasoconstriction).
Nursing Management
Nursing management of the patient in the acute/intermediate phase is focused on the following priorities: restoring fluid balance, preventing infection, modulating hypermetabolism, promoting skin integrity, relieving pain and discomfort, promoting mobility, strengthening coping strategies, supporting patient and family processes, and monitoring and managing complications.
Restoring Normal Fluid Balance
- Daily weights and careful calculation of intake and output are utilized to guide therapy. Thirst, a normal body response to hypovolemia, may cause the patient to drink excessive amounts of water, resulting in dilutional hyponatremia. Changes in physical assessment and hemodynamic indicators are also useful in evaluating the patient’s response to treatment.
Preventing Infection
Increased temperature, tachycardia, tachypnea, and leukocytosis are inherently present in patients with burns, masking clinical signs of infection. A major part of the nurse’s role during the acute phase of burn care is detection and prevention of infection.
- Provide a clean environment, including the promotion of protective isolation interventions. The patient is protected from sources of contamination, including other patients, staff members, visitors, and equipment.
- Migration of microorganisms can occur as the patient touches their wounds or dressings, or from bed sheets that become colonized by microorganisms or contaminated with feces. Regular bathing of unburned areas and changing of linens can help prevent infection.
- Fresh flowers, plants, and fresh fruit baskets are not permitted in the patient’s room because of the risk of microorganism growth.
- Changing invasive lines and tubing routinely in accordance with Centers for Disease Control and Prevention (CDC) recommendations and institutional policy, and prompt removal when no longer indicated, will prevent many HAIs.
Modulating Hypermetabolism
- Collaboration with the dietitian or nutrition support team helps meet the needs of the patient. High-calorie nutritional supplements and vitamin and mineral supplements may be required. Accurate documentation of nutritional intake helps manage treatment.
- Insertion of a feeding tube with continuous or bolus feedings of specific formulas is indicated for if oral feedings are inadequate.
- Daily weight is tracked to properly assess appropriate weight parameters and to attenuate catabolism of lean muscle mass.
Promoting Skin Integrity
- Wound care is usually the single most time-consuming element of burn care after the emergent phase. The primary provider prescribes the desired topical antibacterial agents and specific wound coverings and plans for surgical excision and grafting.
- The nurse needs to make astute assessments of wound status, use creative approaches to dressing of wounds, and support the patient during the emotionally distressing and significantly painful experience of wound care.
- Important wound assessment features include size, color, odor, presence of eschar and exudate, epithelial buds (small pearl-like clusters of cells on the wound surface), bleeding, granulation tissue, the status of graft take, healing of the donor site, and the condition of the surrounding skin. Any significant changes are reported because they may indicate burn wound infection and require immediate intervention.
- The nurse assists the patient and family by providing education, support, and encouragement to take an active part in dressing changes and wound care when appropriate.
- Discharge planning needs for wound care must be anticipated early in the course of burn management, and the strengths of the patient and family are assessed and used in preparing for the patient’s eventual discharge and home care needs. Family presence during dressing changes promotes feelings of readiness for discharge.
Relieving Pain and Discomfort
- Frequent assessment of pain is required, and analgesic and anxiolytic medications are administered as prescribed. Analgesia is best administered before pain becomes severe. Nonpharmacologic interventions help moderate pain.
- Postburn pruritus affects almost all patients with burns and is one of the most distressing symptoms in the postburn period. Oral antipruritic agents, environmental conditions, frequent lubrication of the skin with water or silica-based lotion, and diversion activities all help to promote comfort in this phase. The instructions “pat, don’t scratch” must be reinforced to prevent further discomfort and infectious complications.
- Sleep aids may be prescribed on a regular basis in addition to analgesic and anxiolytic agents as lack of sleep and rest interfere with healing, comfort, and restoration of energy.
Promoting Physical Mobility
An early priority is prevention of the complications of immobility.
- Deep breathing, turning, and proper positioning are essential nursing practices that prevent atelectasis and pneumonia, control edema, and prevent pressure injuries and contractures.
- Early mobility is strongly encouraged. If the lower extremities are burned, elastic pressure bandages are applied prior to placing the client in an upright position in order to promote venous return and minimize edema formation.
- The burn wound is in a dynamic state for at least 1 year after wound closure. During this time, aggressive efforts must be made to prevent contracture and hypertrophic scarring. Both passive and active range-of-motion exercises are initiated from the day of admission and are continued after grafting within prescribed limitations. Splints or functional devices applied to the extremities may lessen contractures through compression and stretch. The nurse monitors the splinted areas for signs of vascular insufficiency, nerve compression, and skin breakdown. Occupational and physical therapists are consulted to develop a patient-specific plan of care throughout hospitalization and recovery.
Strengthening Coping Strategies
- Little emotional energy is left for coping in lieu of maintaining vital physical functions and wound healing. Grief, depression, anger, regression, and manipulative behavior are common responses of patients who have burn injuries as they face the reality of the burn injury. One way to help the patient handle these emotions is to enlist someone to whom the patient can express feelings without fear of retaliation. A nurse, social worker, psychiatric liaison nurse, peer supporter, spiritual advisor, or counselor who is not involved in direct care activities may fill this role successfully.
- Even when physically unable to contribute much to self-care, they should be included in decisions regarding care and encouraged to assert their individuality in terms of preferences and recognition of their unique identities. As the patient improves in mobility and strength, the nurse works with the patient to set realistic expectations for self-care and planning for the future. Contractual agreements help recognize independence, set expectations, and encourage positive communication.
Supporting Patient and Family Processes
- The life-altering burn injury has tremendous psychological, economic, and social impact on the patient and family. Referrals should be made as appropriate.
- Because burn injuries are sudden and unexpected, family roles are disrupted. Therefore, both the patient and the family need thorough information regarding the patient’s burn care and expected course of treatment.
Monitoring and Managing Potential Complications
| Complication | Management |
|---|---|
| Acute Respiratory Failure Acute Respiratory Distress Syndrome | Monitor respiratory status closely and its potential manifestations, including indications for at-risk pulmonary status and signs of cerebral hypoxia. Medical management may require intubation and mechanical ventilation if not already in use. In ARDS, higher oxygen levels, positive end-expiratory pressure, and pressure support promote gas exchange across the alveolar-capillary membrane. |
| Heart Failure Pulmonary Edema | Assess for signs of heart failure (↓ CO, oliguria, jugular vein distension, persistent edema, and the onset of an S₃ or S₄ heart sound). Invasive hemodynamic monitoring shows increased central venous, pulmonary artery, and pulmonary artery wedge pressures in increased fluid volume. Assess for signs of pulmonary edema. Crackles and increasing dyspnea should be reported. The patient is positioned the head of the bed raised (if not contraindicated) to promote lung expansion and gas exchange. Provide supplemental oxygen, and administer IV diuretic and vasoactive agents if indicated and carefully assess the patient’s response. |
| Sepsis | Sepsis is the leading cause of morbidity and mortality in patients with burn injuries. The signs of early sepsis are subtle and masked by the hypermetabolic status. |
| Delirium | Delirium, a transient and often reversible state of acute brain dysfunction, manifests as alterations in consciousness or cognitive function compared to the patient’s baseline. Symptoms include restlessness, disorientation, sleep disorders, or anxiety; some patients experience hallucinations, delusions, or even become combative or suicidal. |
Rehabilitation Phase
Rehabilitation begins immediately after the burn has occurred and often extends for years after the initial injury. An important focus of the burn team is to evaluate for late complications related to burn injuries:
| Complications | Contributing Factors | Interventions |
|---|---|---|
| Neuropathies and nerve entrapment | Electrical injury, large deep burns, improper positioning, edema, scar tissue | Assess peripheral pulses and sensation (neurovascular checks). Prevent edema and pressure by elevation, positioning, and prevention of constricting dressings. Assess splint for proper fit and application. Consult OT and PT departments of positioning. |
| Wound breakdown and/or pressure injury formation | Shearing, pressure, inadequate nutrition | Protect wound from pressure and shearing forces. Educate patient about importance of good nutrition. |
| Hypertrophic scarring | Partial- and full-thickness burns | Keep skin pliable and soft by using emollients. Apply pressure garments as prescribed. Massage. |
| Contractures | Partial- and full-thickness burns | Maintaining position of joints in alignment. |
| Joint instability | Burn wound, burn scar, and contractures | Maintain appropriate joint positioning through appropriate application of splints. Monitor joint pinning if indicated. |
| Complex pain | Trauma and burns | Provide adequate pain management. Consult OT and PT departments for exercises and desensitization. Promote gentle motion of affected extremities. |
Individualized plans of care that are specific to the severity and location of injury are developed and reevaluated frequently. The ultimate goal is to return patients to the highest level of function possible within the context of their injuries. Specially trained occupational and physical therapists are essential for optimal patient outcomes.
Psychological Support
A patient’s outlook, motivation, and support system are important to their overall well-being and ability to progress through the rehabilitation phase. The life-altering nature of burn injuries almost always causes temporary or permanent impairment of psychosocial adaptation.
- In the acute phase of the injury, acute shock, terror, disbelief, confusion, and anxiety are common. Patients may be at risk for delirium and may experience temporary psychoses.
- Patients may be confused from medications they are taking, but they have an underlying sense of fear, anxiety, and pain.
- Patients may experience devastating grief and loss. The sense of loss may originate from physical injury, loss of control from the forced dependency on others for care, or loss of family members/friends who may have died from burn injuries. In residential fires, survivors may have lost their homes and all of their possessions.
- Posttraumatic stress disorder (PTSD) is a common psychiatric disorder in patients with burns. Patients with PTSD re-experience the injury event, exhibit an intensified perception of threat, and employ avoidance behaviors that sustain the symptoms.
- Organizations that provide support for reintegration are able to offer education and training geared specifically to patients with burn injuries. Workshops on how to apply makeup to reduce the appearance of scars can benefit those with obvious facial scarring.
Abnormal Wound Healing
Deeper wounds will likely develop scarring of variable degrees. There are modifiable and nonmodifiable (e.g., heredity) risk factors related to scar formation. The focus of nurses are on modifiable risk factors. Normal scarring occurs in a superficial tissue injury and begins forming within 7 to 10 days post injury and progresses over the next 6 to 12 months. Abnormal scarring occurs after a longer period of wound healing and may form either hypertrophic or keloid scars.
- Hypertrophic scars form within the boundaries of the initial wound and push outward on the perimeter of the wound. They are common in areas over joints and in the younger population. The scar becomes red (due to its hypervascularity), raised, and hard.
- Keloid scars are irregularly formed and extend beyond the margins of the original wound. They are nodular, ropelike, often causing itching and tenderness. They are more common in dark-pigmented skin, uncommon in children and older adults, and have familial tendencies.
- Compression is introduced early in burn wound treatment. Application of elastic pressure garments loosens collagen bundles and encourages parallel orientation of the collagen to the skin surface. As pressure continues over time, collagen restructures and vascularity decreases.
- Elastic bandage wraps used initially help promote adequate circulation, but they can also be used as the first form of compression for scar management, followed by elasticized tubular bandages until the patient can be measured for a customized garment.
- There is some controversy for this therapy, but pressure has been shown to be beneficial in controlling scar formation over time. Recommended garment wear time is 23 hours per day; removing for bathing or wound care only.
- Many areas of the body are difficult to compress due to the contours or location of the injury. Inserts, such as silicone sheets, are helpful for these small troublesome areas and are placed beneath the garment or compression dressing to enhance scar compression.
- Gentle superficial scar massage can be performed with a moisturizer several times a day.
- Burn reconstruction is a treatment option after scars have matured and is discussed within the first few years after injury. This decision requires individualized planning, realistic expectations, and patience. The treatment team and the patient will ultimately decide on the best approach for long-term functionality and cosmesis.
Nursing Management
Ongoing physical assessments related to rehabilitation goals include range of motion of affected joints, functional abilities in ADLs, early signs of skin breakdown, evidence of neuropathies (nerve damage), activity tolerance, and quality or condition of healing skin. The patient’s participation in care and ability to demonstrate self-care in such areas as ambulation, eating, wound cleaning, toileting, and applying pressure wraps are documented on a regular basis.
The major goals for the patient include increased mobility and participation in ADLs; adaptation and adjustment to alterations in body image, self-concept, and lifestyle; increased understanding and knowledge of the injury, treatment, and planned follow-up care; and absence of complications.
Nursing Diagnoses, Goals, and Interventions
- Activity intolerance associated with pain with exercise, limited joint mobility, muscle wasting, and limited endurance. Goal: Increased mobility and participation in ADLs.
- Rehabilitation can be painful and challenging. Strategies to maintain motivation and participation may be beneficial during this critical phase.
- The patient’s activity tolerance, strength, and endurance gradually increase if activity occurs over increasingly longer periods. Monitoring of fatigue and pain tolerance will assist with determining the amount of activity to be encouraged on a daily basis.
- The nurse must schedule care in such a way that the patient has periods of rest and uninterrupted sleep. A good time for planned patient rest is after the stress of dressing changes and exercise, while pain interventions and sedatives are still effective. Family members and other care providers are informed of this plan to prevent disturbances. In patients with insomnia related to frequent nightmares about the burn injury or other fears and anxieties, the nurse may provide reassurance and agents, as prescribed, to promote sleep.
- Reducing metabolic stress by relieving pain, preventing chilling or fever, and promoting the physical integrity of all body systems helps the patient conserve energy for therapeutic activities and wound healing.
- Disturbed body image associated with altered physical appearance and self-concept. Goals: Adaptation and adjustment to alterations in body image, self-concept, and lifestyle.
- The healthcare team must actively promote a healthy body image and self-concept in patients with burn injuries so that they can accept or challenge others’ perceptions of those who are disfigured or disabled. Survivors themselves must show others who they are, how they function, and how they want to be treated.
- Impaired mobility due to contractures or hypertrophic scarring. Goal: Increased mobility.
- Early and aggressive physical and occupational therapy makes contractures or hypertrophic scars a rare long-term complication.
- Surgical intervention is indicated if full range of motion in the patient with burns is not achieved.
- Lack of knowledge about postdischarge home care and recovery needs. Goal: Increased understanding and knowledge of the injury, treatment, and planned follow-up care
- (Collaborative) Inadequate psychological adaptation to burn injury. Goal: Absence from complications.
- Psychological counseling or psychiatric referral may be made to assess the patient’s emotional status, to help the patient develop coping skills, and to intervene if major psychological issues or ineffective coping is identified.
Outpatient Burn Care
The goals for treatment in an outpatient setting may include burn wound management, pain management, scar and reconstructive care, psychosocial care, and rehabilitation.
- The initial outpatient visit for a discharged patient with burn injuries is usually scheduled within 3 to 5 days after hospital discharge. A survivor’s follow-up appointment schedule will vary and decrease in frequency over time, based on patient’s needs.
- Patient and family education is paramount and should include verbal and written instructions as well as return demonstration of the wound or scar care required. Emphasis should be placed on the importance of keeping follow-up appointments and notification about changes in symptoms.
- Physical and occupational therapy are often provided in the outpatient burn setting. The rehabilitation goals are to increase range of motion, strengthen muscles, and build the patient’s activity tolerance through a specific, individualized plan of care that includes routine visits for up to 2 years or more following the injury.
- The patient’s adaptation to lifestyle changes and emotional status should be assessed during the outpatient visits and proper referrals made for counseling services. It is helpful to incorporate family response and interactions into the assessment. The healthcare team must also be alert to issues of substance abuse, safety concerns, suicidal thoughts, depression, and PTSD.