Reference:
- Brunner & Suddarth’s Textbook of Medical-Surgical Nursing, 15th Edition, ISBN 978-197-51-6103-3, by Janice L. Hinkle, Kerry H. Cheever, and Kristen J. Overbaugh (pp. 2055-2060)
- Saunders Comprehensive Review for the NCLEX-RN Examination, 9th Edition, ISBN 978-032-37-9530-2, by Linda Anne Silvestri, Angela E. Silvestri, and Jessica Grimm (Ch. 59, pp. 859-860)
Traumatic head injury is the leading cause of death and disability from ages 1 to 44, at an annual rate of ~52,000 deaths due to TBI, with two-thirds of that population being men. It is caused by an external mechanical force and may result in permanent or temporary impairment of cognitive, physical, and psychosocial functions, with an associated diminished or altered state of consciousness. These forces may occur from falls, collisions (vehicles, other moving objects such as a baseball), violence (gunshots, abuse, shaken baby syndrome), sports injuries, etc.
Types of TBI
- Closed: the skull is not broken; the brain is not exposed. This may be due to rapid movement such as in sudden accelerations or decelerations. Depending on which region the brain hits, this may be considered as a coup (frontal) contusion from deceleration or sudden hyperextension of the head, or contrecoup (occipital) contusion from acceleration or sudden hyperflexion of the head.
- Concussion: temporary loss of consciousness; widespread and microscopic jarring of the brain within the skull.
- Contusions: localized, macroscopic, and “bruising” type of injury. Noticeable loss of function is noted. Coup-contra coup involvement. Bruising occurs, and the brain stem may swell and tear.
- Fractures: hairline (a line, no splintering and distortion), depressed (crushed portion of skull), compound (break in skin, splintering of bone), comminuted (fragmentation)
- Basilar skull fracture: a fracture on the base of the skull. This manifests as rhinorrhea and otorrhea from CSF leakage, raccoon eyes (ecchymosis around the eye), and battle’s sign (ecchymosis behind the ear). On a pillow, a “halo ring” is formed by a stain of CSF with blood in the center.
- Open: a penetrating head injury which may be focal (isolated to one area) or diffuse (widespread).
Monro-Kellie Doctrine
According to the Monro–Kellie hypothesis, the cranial vault is a closed system, and if one of the three components (brain, blood, cerebrospinal fluid) increases in volume, at least one of the other two must decrease in volume or the pressure will increase.
Any bleeding or swelling within the skull increases the volume of contents within the skull and therefore causes increased intracranial pressure (ICP). If the pressure increases enough, it can cause displacement of the brain through or against the rigid structures of the skull. This causes restriction of blood flow to the brain, decreasing oxygen delivery and waste removal. Cells within the brain become anoxic and cannot metabolize properly, producing ischemia, infarction, irreversible brain damage, and eventually brain death
The damage caused by a traumatic brain injury, i.e. it’s pathophysiology, begins with the primary injury, literally the damage caused by the trauma at the moment of injury. The secondary injury is the damage produced after the initial trauma, such as rebound contusions (the brain bounces back onto the contrecoup after hitting the coup), swelling, increased ICP, hypoxia, etc.
- Primary Brain Damage: due to two main mechanisms (a) contact, e.g. an object striking the head producing fractures or contusions, and (b) change in momentum, i.e. sudden acceleration and deceleration producing shear, tensile, and compressive strains on the brain. These may result in intracranial hematoma (most common cause of death in TBI), diffuse vascular injury, and injury to the cranial nerves and pituitary stalk.
Intracranial Hemorrhage
An intracranial hemorrhage is classified according to its location:
- Epidural Hematoma: bleeding from a fracture of the temporal bone and rupture of the middle meningeal artery.
- Subdural Hematoma: bleeding from ruptured bridging veins in the subdural space.
- Subarachnoid Hemorrhage: bleeding from damage to blood vessels in the posterior fossa stalk.
- Intracerebral Hemorrhage: bleeding within the brain
- Intraventricular Hemorrhage: bleeding into the ventricles of the brain
- Secondary Brain Injury: occurring hours or days after the initial injury, this may result from impairment in cerebral blood flow due to local edema, hemorrhage, increased intracranial pressure such, shock, disturbance of pulmonary ventilation (aspiration, chest wall instability, neurogenic disturbance), etc.
- Decreased perfusion results in cellular destruction, causing neuronal death.
Clinical Manifestations
Symptoms, apart from those of the local injury, depend on the severity and the anatomic location of the underlying brain injury. Persistent, localized pain usually suggests that a fracture is present.
- Cognitive Changes: change in level of consciousness (loss of consciousness, speech, lethargy, attention deficit, mood disturbances), memory, learning, problem-solving, speed of mental processing, judgment, and decision-making.
- Attention deficits, changes in sleep habits, and mood disturbances may be found in children with TBI, along with changes in eating habits and persistent, inconsolable crying.
- Physical Changes: weakness or numbness in the extremities; persistent, potentially worsening headache, spasticity, physical paralysis, chronic pain, changes in sensorium, loss of stamina, and loss of control of the bowel and bladder.
Fractures of the Cranial Vault
Fractures of the cranial vault may or may not produce swelling in the region of the fracture.
- Fractures of the base of the skull tend to traverse the paranasal sinus of the frontal bone or the middle ear located in the temporal bone. Therefore, they frequently produce hemorrhage from the nose, pharynx, or ears, and blood may appear under the conjunctiva. An area of ecchymosis (bruising) may be seen over the mastoid (Battle sign).
- Basal skull fractures are suspected when CSF escapes from the ears (CSF otorrhea) and the nose (CSF rhinorrhea). Drainage of CSF is a serious problem, because meningeal infection can occur if organisms gain access to the cranial contents via the nose, ear, or sinus through a tear in the dura.
Categorized into severity of TBI:
- Mild TBI: loss of consciousness for seconds to minutes, problems with memory or concentration, headache, dizziness/loss of balance, nausea/vomiting, and difficulty sleeping
- Moderate to Severe TBI: loss of consciousness for minutes to hours, problems with speech, inability to awaken from sleep, weakness or numbness in the extremities or digits, loss of coordination (ataxia), and persistent, worsening headache.
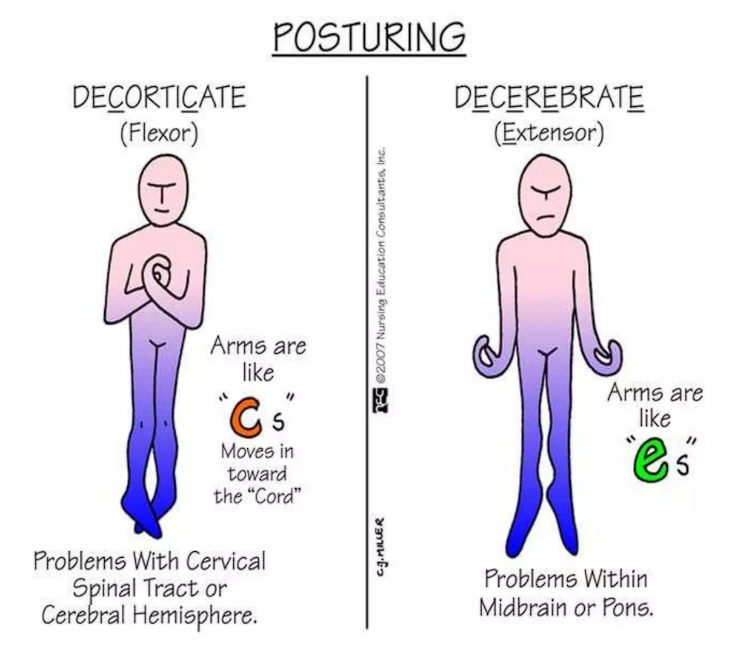
Posturing
Individuals with severely injury may experience decorticate or decerebrate posturing:
- Decorticate: the arms are rigidly flexed at the elbows and wrists, with the legs possible flexed with the toes rigidly pointed. This indicates a lesion in the brain, and may sometimes be produced by applying a painful stimulus to a comatose patient. In Glasgow’s coma scale, this finding would be rated as a 3/6 on the motor scale.
- Decerebrate: the arms are rigidly straight and internally rotated. The legs are extended with the toes rigidly pointed. This is usually observed in patients afflicted by compression of the brain stem at a low level. In Glasgow’s coma scale, this finding would be rated as a 2/6 on the motor scale.
The progression of a patient from a decorticate posture to a decerebrate posture indicates worsening of their condition, as reflected by Glasgow’s coma scale. The most severe posturing is flaccid posturing, the absence of motor response in any extremity.
Increased Intracranial Pressure
- Altered level of consciousness, which is the most sensitive and earliest indication of increasing ICP
- Headache
- Abnormal respirations: Cheyne-Stokes, neurogenic hyperventilation, apneustic, ataxic, cluster
- Rise in blood pressure with widening pulse pressure
- Slowing of pulse
- Elevated temperature
- Vomiting
- Pupil changes
- Late signs of increased ICP include increased systolic blood pressure, widened pulse pressure, and slowed heart rate. These, along with abnormal respirations, completes the Cushing triad/Cushing reflex.
- Other late signs include changes in motor function from weakness to hemiplegia, a positive Babinski’s reflex, decorticate or decerebrate posturing, and seizures.
Assessment and Diagnostic Findings
Computed tomography (CT) scan can be used to diagnose a skull fracture. This may be difficult depending on the site of fracture. Once a diagnosis is made, the patient is assessed for associated brain injury. Magnetic Resonance Imaging (MRI) scans provide better resolution and clearer pictures of the injured area.
Complications
An altered level of consciousness is highly representative of worsening conditions in the brain for a patient with traumatic brain injury. These may appear in varying degrees:
- Coma: the person is fully unconscious, resulting from widespread damage to all parts of the brain. It may take days to weeks for a person to emerge from a coma, after which they may still remain in a vegetative state.
- Vegetative State: a potentially permanent state wherein individuals are physically awake, but show no signs of cognition.
- Minimally Conscious State: a severely altered level of consciousness but with some evidence of self and environmental awareness.
- Locked-In Syndrome: a condition where an individual’s consciousness is intact, but they are unable to speak or move, often only being able to communicate with eye movement or blinking.
Other complications include :
- Infections, a consistent problem in patients with skull fractures or other openings or entry points.
- Blood Vessel Damage from the injury, which can result in strokes or clotting.
- Nerve Damage, specifically the cranial nerves that arise directly from the brain, can result in facial paralysis, loss of vision, and dysfunction related to other cranial nerves.
Medical Management
Operative management is not used to correct brain injury. It is only used to address (a) the need for ICP monitoring with a bolt or other device; (b) bleeding within the brain—surgical removal or drainage may be necessary; and (c) removal of skull bone fragments/damaged tissue (débridement) and repair of skull fractures if present in open or depressed head injuries. This is usually done within 24 hours of injury.
- Craniotomy: removal of tumor, relieve ICP, remove blood clots, or control hemorrhage. This may be (a) supratentorial, (b) infratentorial, or (c) transsphenoidal.
- Alternative: craniectomy and cranioplasty
In nondepressed skull fractures, surgical treatment is not necessary, but close observation of the patient is essential. This may be done in the hospital, but if no underlying brain injury is present, the patient may be allowed to return home. The patient and their significant others are given specific instructions for monitoring.
Pharmacologic Management
| Indication | Treatment |
|---|---|
| Increased intracranial pressure | Diuresis |
| Seizure activity | Anti-seizure drugs. This is used prophylactically during the first week of management. |
| Medical induction of a coma | Done to reduce the oxygen demands of the brain, reducing the potential for cell death in hypoperfusion. |
| Problems with attention and concentration | Amantadine, Methylphenidate, Bromocriptine, Antidepressants |
Nursing Management
The nurse primarily focuses her efforts on maintaining a patent airway, ventilation, vital signs, neuro checks, and monitoring for complications (Increasing ICP, Seizures, Hyperthermia)
- Observe for CSF Leak: halo ring appearance of stains. If observed, instruct patient not to blow the nose, elevate the head of bed by 30 degrees, observe for infection (meningitis), place cotton ball on ear to absorb otorrhea, and gauze pad at the bottom of the nose for rhinorrhea.
- Prevent complications of immobility.
- Check for signs of infection.
- Postoperative Positioning:
- Supratentorial positioning: neutral neck alignment and side-lying or supine. Avoid operative side.
- Infratentorial positioning: maintain straight neck alignment; no flexion to avoid tearing suture. Position patient on either side, not supine.
- Transsphenoidal positioning: nasal packing, instruct patient to avoid blowing the nose. Provide oral care and keep head of bed elevated.
Interventions for Increased Intracranial Pressure
- For the client with increased ICP, elevate the head of the bed 30 to 40 degrees, avoid the Trendelenburg’s position, and prevent flexion of the neck and hips.
- Monitor respiratory status and prevent hypoxia.
- Monitor ICP if a pressure device is in place.
- Avoid the administration of morphine sulfate to prevent the occurrence of hypoxia.
- Maintain mechanical ventilation as prescribed; maintaining the PaCO2 at 30 to 35 mm Hg will result in vasoconstriction of the cerebral blood vessels, decreased blood flow, and therefore decreased ICP.
- Maintain body temperature.
- Prevent shivering, which can increase ICP.
- Decrease environmental stimuli.
- Monitor electrolyte levels and acid–base balance.
- Monitor intake and output.
- Limit fluid intake to 1200 mL/day.
- Instruct the client to avoid straining activities, such as coughing and sneezing.
- Instruct the client to avoid Valsalva’s maneuver.