The kidneys, two bean-shaped located retroperitoneally, are the primary organs of the genitourinary system.
- The functional unit of the kidneys are nephrons, containing a network of minute capillaries that filter the blood.
- There are two major functions performed by the kidneys:
- Excretory, i.e., urine formation. This occurs in phases:
- Non-excretory
Physiology of the Kidney and Urinary Systems
Urine Formation
Urine formation occurs through a complex three-step process: glomerular filtration, tubular reabsorption, and tubular secretion. The various substances normally filtered by the glomerulus, reabsorbed by the tubules, and excreted in the urine include sodium, chloride, bicarbonate, potassium, glucose, urea, creatinine, and uric acid.
- Glomerular filtration: the normal blood flow through the kidneys is 1000 and 1300 mL/min. As these flow into the glomerulus, filtration of water, electrolytes, and other small molecules occurs. Under normal conditions, about 20% of the blood passing through the glomeruli is filtered into the nephron, amount to about 180 L/day of filtrate.
- Filtration depends on adequate blood flow that maintains a consistent pressure through the glomerulus called hydrostatic pressure. Many factors can alter this blood flow and pressure, including hypotension, decreased oncopressure in the blood, and increased pressure in the renal tubules from an obstruction.
- Tubular reabsorption: In tubular reabsorption, a substance moves from the filtrate back into the peritubular capillaries or vasa recta. Of the 180 L of filtrate that kidneys produce each day, 99% is reabsorbed into the bloodstream, resulting in the formation of 1 to 2 L of urine each day. Although most reabsorption occurs in the proximal tubule, reabsorption occurs along the entire tubule. Filtrate becomes concentrated in the distal tubule and collecting ducts under hormonal influence and becomes urine, which then enters the renal pelvis. In the absence of Tubular reabsorption, volume depletion would rapidly occur.
- Tubular secretion: In tubular secretion, a substance moves from the peritubular capillary blood plasma (blood) into the Tubular lumen (filtrate). Tubular secretion helps with the elimination of potassium, hydrogen ions, ammonia, uric acid, some drugs, and other waste products.
Antidiuretic Hormone
Antidiuretic hormone (ADH), also known as vasopressin, is a hormone that is secreted by the posterior portion of the pituitary gland in response to changes in osmolality of the blood.
- With decreased water intake, blood osmolality tends to increase, stimulating ADH release. ADH then acts on the kidney, increasing reabsortion of water and thereby returning the osmolality of the blood to normal.
- With excess water intake, the secretion of ADH by the pituitary is suppressed; therefore, less water is reabsorbed by the kidney tubule, leading to diuresis (increased urine volume).
- A dilute urine with a fixed specific gravity (about 1.010) or fixed osmolality (about 300 mOsm/L) indicates an inability to concentrate and dilute the urine, which is a common early sign of kidney disease.
Osmolarity and Osmolality
Osmolarity is the ratio of solute to water. The regulation of salt and water is paramount for control of the extracellular volume and both serum and urine osmolarity. Osmolarity and ionic composition are maintained by the body within very narrow limits. As little as a 1% to 2% change in the serum osmolarity can cause a conscious desire to drink and conservation of water by the kidneys.
Osmolality is the number of osmoles (measure of osmotic pressure) dissolved per kilogram of solution. The filtrate in the glomerular capillary normally has the same osmolality as the blood (280 to 300 mOsm/kg).
Regulation of Water Excretion
A person normally ingest about 1300 mL of oral liquids and 1000 mL of water in food per day. Of the fluid ingested, approximately 800 mL is lost through the skin and lungs and 200 mL through feces (called insensible loss). It is important to consider all fluid gained and lost when evaluating total fluid status. Daily weight measurements are a reliable means of determining overall fluid status. In terms of fluids, one kilogram equals approximately 1000 mL. Therefore, a change in weight of 1 kg could suggest an overall fluid gain or loss of 1000 mL.
Regulation of Electrolyte Excretion
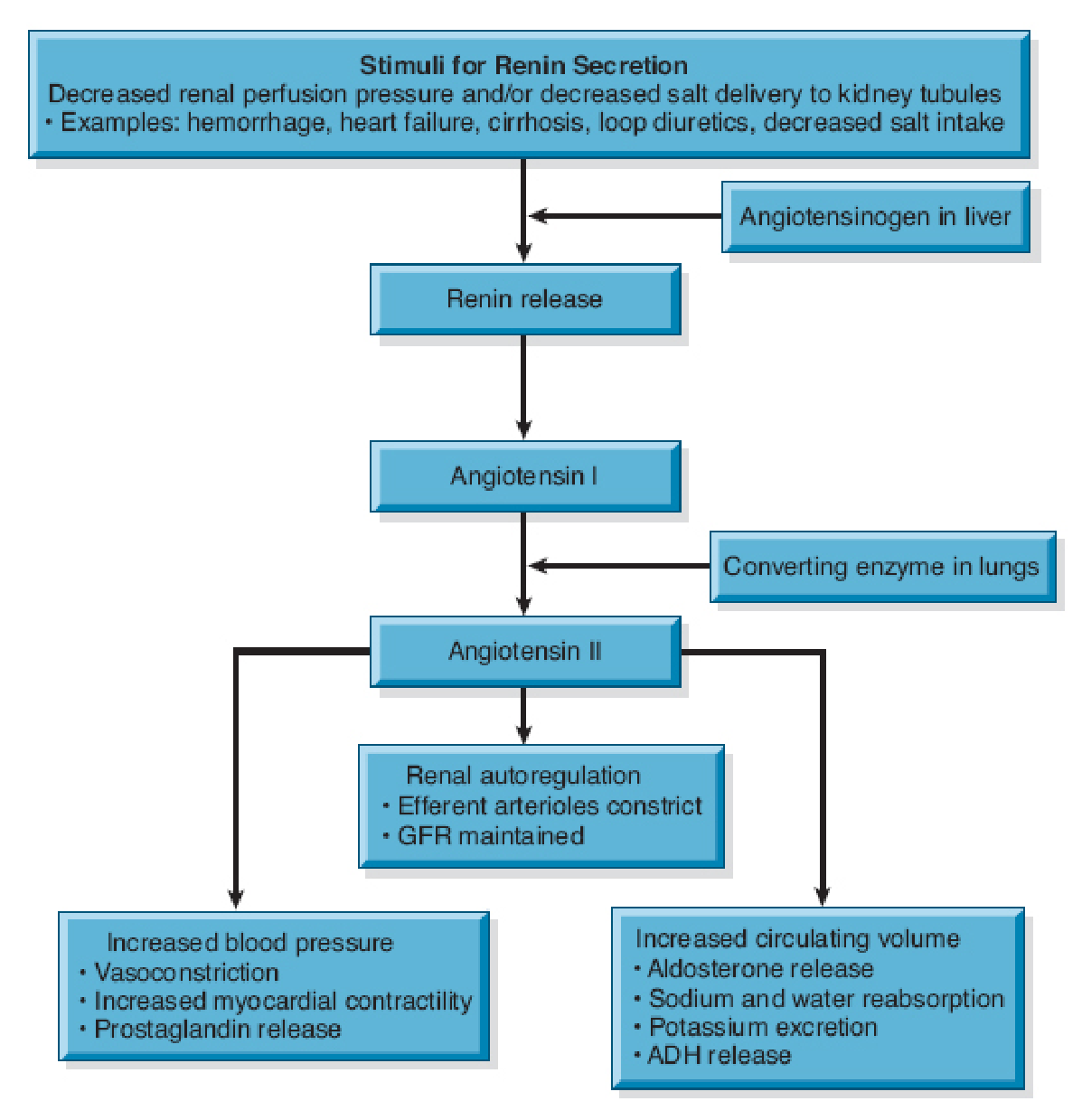
Electrolyte intake and excretion is normally equal. The regulation of sodium volume excreted depends on aldosterone, a hormone synthesized and released by the adrenal cortex. Increased aldosterone reduces sodium excretion as it fosters renal reabsorption of sodium.
- Release of aldosterone from the Adrenal cortex is largely under the control of angiotensin II.
- Angiotensin II levels are in turn controlled by renin, an enzyme that is released from specialized cells in the kidneys.
- This complex system is activated when pressure in the renal arterioles falls below normal levels, as occurs with shock, dehydration, or decreased sodium chloride delivery to the tubules. Activation of this system increases the retention of water and expansion of the intravascular fluid volume, thereby maintaining enough pressure within the glomerulus to ensure adequate filtration.
Regulation of Acid-Base Balance
The normal serum pH is about 7.35 to 7.45 and must be maintained within this narrow range for optimal physiological function. Acids are formed through catabolism or absorbed from the diet. The kidney performs major functions to assist in this balance.
- Reabsorb and return to the body’s circulation any bicarbonate from the urinary filtrate
- Excrete or reabsorb acid, synthesize ammonia, and excrete ammonium chloride.
- Because bicarbonate is a small ion, it is freely filtered at the glomerulus. The renal tubules actively reabsorb most of the bicarbonate in the urinary filtrate. To replace any lost bicarbonate, the renal tubular cells generate new bicarbonate through a variety of chemical reactions. This newly generated bicarbonate is then reabsorbed by the tubules and returned to the body.
- Hydrogen ions can be excreted or reabsorbed in the urine. Excretion can occur directly until urine pH reaches 4.5, which is 1000 times more acidic than blood.
- More acid that needs to be eliminated that cannot be eliminated directly are bound to chemical buffers (e.g., phosphate ions, ammonia) then excreted in the urine.
Autoregulation of Blood Pressure
- Vasa recta are specialized vessels of the kidney that constantly monitor blood pressure as blood begins its passage into the kidney.
- If the vasa recta detect a decrease in blood pressure, specialized juxtaglomerular cells near the afferent arteriole, distal tubule, and efferrent arteriole secrete the hormone renin. Renin converts angiotensinogen to angiotensin I, which is then converted to angiotensin II, the most powerful vasoconstrictor known; angiotensin II causes the blood pressure to increase.
- Increased blood pressure suppresses renin production. Failure of this feedback mechanism is one of the primary causes of hypertension.
Renal Clearance
Regulation of Red Blood Cell Production
When the kidneys detect a decrease in the oxygen tension in renal blood flow, because of anemia, arterial hypoxia, or inadequate blood flow, they release erythropoietin. Erythropoietin is a glycoprotein from the kidney that stimulates the bone marrow to produce RBCs, which carry oxygen throughout the body.
Vitamin D Synthesis
The kidneys are also responsible for the final conversion of inactive vitamin D to its active form, 1,25-dihydroxycholecalciferol. Vitamin D is necessary for maintaining normal calcium balance in the body.
Secretion of Prostaglandins and Other Substances
The kidneys also produce prostaglandin E and prostacyclin, thromboxanes, and leukotrienes, which have vasoactive effects. These substances help the afferent and efferrent arterioles maintain renal blood flow by causing selective vasodilation or vasoconstriction.
Excretion of Waste Products
The kidneys eliminate the body’s metabolic waste products. The major waste product of protein metabolism is urea, of which about 25 to 30 g are produced and excreted daily. All of this urea must be excreted in the urine; otherwise, it accumulates in body tissues. Other waste products of metabolism that must be excreted are creatinine, phosphates, and sulfates. Uric acid, formed as a waste product of purine metabolism, is also eliminated in the urine. The kidneys serve as the primary mechanism for excreting drug metabolites.